Clinical Features and Computed Tomography Characteristics of Non-Klebsiella pneumoniae Liver Abscesses in Elderly (>65 Years) and Nonelderly Patients
- Affiliations
-
- 1Department of Radiology, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan, Republic of China. weichou.chang@gmail.com
- 2Division of General Surgery, Department of Surgery, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan, Republic of China.
- 3Department of Emergency Medicine, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan, Republic of China.
- KMID: 2070033
- DOI: http://doi.org/10.3349/ymj.2015.56.2.519
Abstract
- PURPOSE
To compare the clinical and computed tomography (CT) appearances of liver abscesses caused by non-Klebsiella pneumoniae bacterial pathogens in elderly and nonelderly patients.
MATERIALS AND METHODS
Eighty patients with confirmed non-Klebsiella pneumoniae liver abscesses (non-KPLAs) were enrolled and divided into two age groups: elderly (age > or =65 years, n=42) and nonelderly (age <65 years, n=38). Diagnosis of non-KPLA was established by pus and/or blood culture. We compared clinical presentations, outcomes, and CT characteristics of the two groups, and performed multivariate analysis for significant variables and receiver-operating-characteristic analysis to determine the cutoff value of abscess diameter for predicting non-KPLA.
RESULTS
Elderly patients with non-KPLA were associated with a longer hospital stay (p<0.01). Regarding etiology, biliary sources had a strong association in the elderly group (p<0.01), and chronic liver diseases were related to the nonelderly group (p<0.01). Non-KPLAs (52.5%) tended to show a large, multiloculated appearance in the elderly group and were associated with bile duct dilatation (p<0.01), compared with the nonelderly group. The abscess diameter (cutoff value, 5.2 cm; area under the curve, 0.78) between the two groups was predicted. In multivariate analysis, underlying biliary tract disease [odds ratio (OR), 3.58, p<0.05], abscess diameter (OR, 2.40, p<0.05), and multiloculated abscess (OR, 1.19, p<0.01) independently predicted elderly patients with non-KPLA.
CONCLUSION
In the elderly patients with non-KPLA, a large, multiloculated abscess with a diameter greater than 5.2 cm was the predominant imaging feature.
Keyword
MeSH Terms
-
Adult
Aged
Aged, 80 and over
Bacterial Infections/*complications/*radiography
Female
Humans
Klebsiella Infections/microbiology
Klebsiella pneumoniae
Length of Stay
Liver Abscess/complications/microbiology/*radiography
Logistic Models
Male
Microscopy
Middle Aged
Multivariate Analysis
ROC Curve
Retrospective Studies
Tomography, X-Ray Computed/*methods
Figure
-

Fig. 1 A 72-year-old woman with non-KPLA (caused by Enterococcus) who presented with fever and right upper quadrant pain for 7 days. An axial, contrast-enhanced CT image (A) shows a large (size: about 7.9 cm) abscess (arrows) in the dome. A coronal, contrast-enhanced reconstruction CT image (B) shows the abscess with a multiloculated appearance (arrow), which was associated with bile duct dilatation (star) and pneumobilia (arrowhead). Acute cholecystitis was found. This was the most common appearance of liver abscess in the elderly. Note also the mild bilateral pleural effusions and basal atelectasis. The patient received antibiotics and PCD drainage, and she was discharged after 25 days. KPLA, Klebsiella pneumoniae liver abscess; PCD, percutaneous catheter drainage.
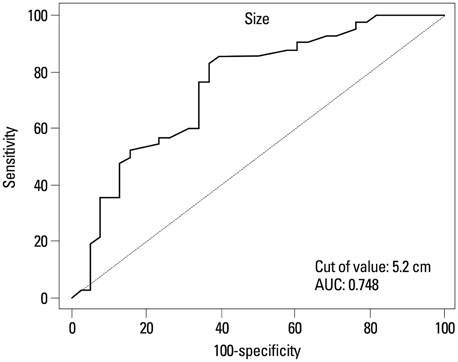
Fig. 2 Receiver-operating-characteristic (ROC) analysis of the minimal diameter for abscesses in the elderly group. AUC, the area under the ROC curve.
Reference
-
1. Foo NP, Chen KT, Lin HJ, Guo HR. Characteristics of pyogenic liver abscess patients with and without diabetes mellitus. Am J Gastroenterol. 2010; 105:328–335.
Article2. Lee NK, Kim S, Lee JW, Jeong YJ, Lee SH, Heo J, et al. CT differentiation of pyogenic liver abscesses caused by Klebsiella pneumoniae vs non-Klebsiella pneumoniae. Br J Radiol. 2011; 84:518–525.
Article3. Alsaif HS, Venkatesh SK, Chan DS, Archuleta S. CT appearance of pyogenic liver abscesses caused by Klebsiella pneumoniae. Radiology. 2011; 260:129–138.
Article4. Yang CC, Yen CH, Ho MW, Wang JH. Comparison of pyogenic liver abscess caused by non-Klebsiella pneumoniae and Klebsiella pneumoniae. J Microbiol Immunol Infect. 2004; 37:176–184.5. Lederman ER, Crum NF. Pyogenic liver abscess with a focus on Klebsiella pneumoniae as a primary pathogen: an emerging disease with unique clinical characteristics. Am J Gastroenterol. 2005; 100:322–331.
Article6. Law ST, Li KK. Older age as a poor prognostic sign in patients with pyogenic liver abscess. Int J Infect Dis. 2013; 17:e177–e184.
Article7. Chen SC, Lee YT, Yen CH, Lai KC, Jeng LB, Lin DB, et al. Pyogenic liver abscess in the elderly: clinical features, outcomes and prognostic factors. Age Ageing. 2009; 38:271–276.
Article8. Alvarez JA, González JJ, Baldonedo RF, Sanz L, Junco A, Rodrfíguez JL, et al. Pyogenic liver abscesses: a comparison of older and younger patients. HPB (Oxford). 2001; 3:201–206.
Article9. Kang SC, Hwang SJ. Impact of advanced age on inpatients with pyogenic liver abscess in Taiwan: a nationwide claim-based analysis. J Chin Med Assoc. 2011; 74:539–543.
Article10. Tan YM, Chung AY, Chow PK, Cheow PC, Wong WK, Ooi LL, et al. An appraisal of surgical and percutaneous drainage for pyogenic liver abscesses larger than 5 cm. Ann Surg. 2005; 241:485–490.
Article11. Lee CH, Leu HS, Wu TS, Su LH, Liu JW. Risk factors for spontaneous rupture of liver abscess caused by Klebsiella pneumoniae. Diagn Microbiol Infect Dis. 2005; 52:79–84.
Article12. Liao WI, Tsai SH, Yu CY, Huang GS, Lin YY, Hsu CW, et al. Pyogenic liver abscess treated by percutaneous catheter drainage: MDCT measurement for treatment outcome. Eur J Radiol. 2012; 81:609–615.
Article13. Tazawa J, Sakai Y, Maekawa S, Ishida Y, Maeda M, Marumo F, et al. Solitary and multiple pyogenic liver abscesses: characteristics of the patients and efficacy of percutaneous drainage. Am J Gastroenterol. 1997; 92:271–274.14. Chou FF, Sheen-Chen SM, Chen YS, Chen MC. Single and multiple pyogenic liver abscesses: clinical course, etiology, and results of treatment. World J Surg. 1997; 21:384–388.
Article15. Liu CH, Gervais DA, Hahn PF, Arellano RS, Uppot RN, Mueller PR. Percutaneous hepatic abscess drainage: do multiple abscesses or multiloculated abscesses preclude drainage or affect outcome? J Vasc Interv Radiol. 2009; 20:1059–1065.
Article16. Barakate MS, Stephen MS, Waugh RC, Gallagher PJ, Solomon MJ, Storey DW, et al. Pyogenic liver abscess: a review of 10 years' experience in management. Aust N Z J Surg. 1999; 69:205–209.
Article17. Lam YH, Wong SK, Lee DW, Lau JY, Chan AC, Yiu RY, et al. ERCP and pyogenic liver abscess. Gastrointest Endosc. 1999; 50:340–344.
Article18. Walsh RM. Innovations in treating the elderly who have biliary and pancreatic disease. Clin Geriatr Med. 2006; 22:545–558.
Article19. Mølle I, Thulstrup AM, Jepsen P, Sørensen HT, Vilstrup H. Liver cirrhosis is risk factor for pyogenic liver abscesses. BMJ. 2001; 323:52–53.20. Tarantino G, Finelli C. What about non-alcoholic fatty liver disease as a new criterion to define metabolic syndrome? World J Gastroenterol. 2013; 19:3375–3384.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Klebsiella Pneumoniae Multi-organ Abscesses not Accompanied by Liver Abscesses: A Case Report
- Lower Leg Abscess in Klebsiella pneumoniae Invasive Syndrome Caused by Hypervirulent Klebsiella pneumoniae: A Case Report
- Two Cases of Bilateral Endogenous Klebsiella pneumoniae Endophthalmitis in Primary Klebsiella pneumoniae Liver Abscess Patients
- A clinical study on pyogenic liver abscesses: the changes in the clinical features during the recent 12 years
- Metastatic endophthalmitis and thyroid abscess complicating Klebsiella pneumoniae liver abscess
