J Korean Soc Radiol.
2015 Oct;73(4):209-215. 10.3348/jksr.2015.73.4.209.
Chest CT Findings in Patients with Non-Cardiovascular Causes of Chest Pain: Focusing on Pulmonary Tuberculosis in a Tuberculosis Endemic Country
- Affiliations
-
- 1Department of Radiology, Mokdong Hospital, Ewha Womans University School of Medicine, Seoul, Korea. sinisim@ewha.ac.kr
- 2Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Mokdong Hospital, Ewha Womans University School of Medicine, Seoul, Korea.
- KMID: 2068710
- DOI: http://doi.org/10.3348/jksr.2015.73.4.209
Abstract
- PURPOSE
To review the common causes of non-cardiovascular chest pain (NCCP) according to the location and lesion type as seen on chest CT, and to evaluate CT findings in tuberculosis (TB) as a cause of NCCP.
MATERIALS AND METHODS
In the period 2009 to 2012, patients having NCCP without definitive evidence of acute myocardial infarction, pulmonary thromboembolism, and aortic dissection, were included. In total, 162 patients (60.5% male; 39.5% female), with a mean age of 51 years, were enrolled. CT images were evaluated by location and lesion type, for causes of NCCP.
RESULTS
Chest CT revealed that the most common location for the cause of NCCP was the pleura (45.1%), followed by the subpleural lung parenchyma (30.2%). The most common lesion causing NCCP was TB (33.3%), followed by pneumonia (19.1%). Of the 54 TB cases, 40 (74.1%) were stable TB and 14 (25.9%) were active TB; among these 54 patients, NCCP was most commonly the result of fibrotic pleural thickening (55.6%), followed by subpleural stable pulmonary TB (14.8%).
CONCLUSION
Results of chest CT revealed that TB was a major cause of NCCP in a TB endemic area. Among the TB patients, fibrotic pleural thickening in patients with stable TB was the most common cause of NCCP.
MeSH Terms
Figure
-
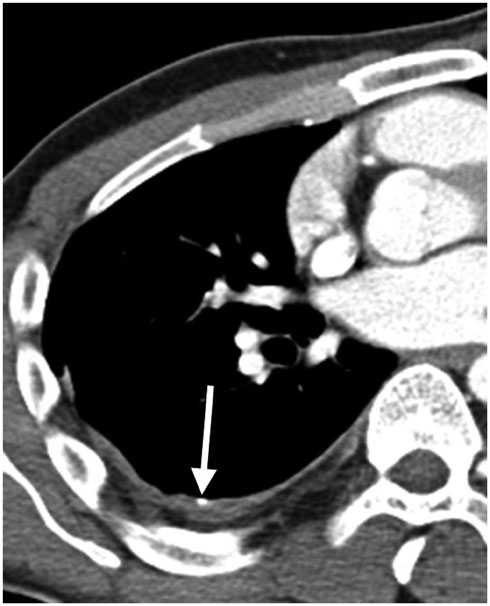
Fig. 1 A 35-year-old man having right posterior chest pain for 30 days. The transaxial CT (3.0-mm collimation, 80 mA) mediastinal window shows benign pleural thickening with calcification (arrow) of the right posterior costal pleura.
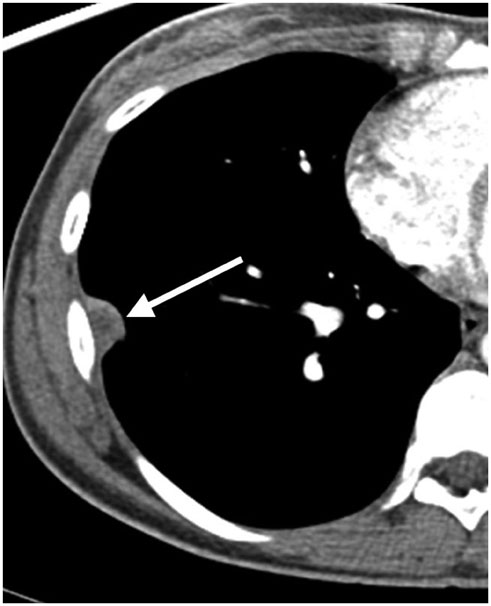
Fig. 2 A 53-year-old woman having right chest pain for 7 days. The transaxial CT (3.0-mm collimation, 80 mA) mediastinal window shows focal empyema (arrow) of the right lateral costal pleura.
Reference
-
1. Ford AC, Suares NC, Talley NJ. Meta-analysis: the epidemiology of noncardiac chest pain in the community. Aliment Pharmacol Ther. 2011; 34:172–180.2. Chierchia SL, Fragasso G. Angina with normal coronary arteries: diagnosis, pathophysiology and treatment. Eur Heart J. 1996; 17:Suppl G. 14–19.3. Chang SA, Choi SI, Choi EK, Kim HK, Jung JW, Chun EJ, et al. Usefulness of 64-slice multidetector computed tomography as an initial diagnostic approach in patients with acute chest pain. Am Heart J. 2008; 156:375–383.4. Rubinshtein R, Halon DA, Gaspar T, Jaffe R, Karkabi B, Flugelman MY, et al. Usefulness of 64-slice cardiac computed tomographic angiography for diagnosing acute coronary syndromes and predicting clinical outcome in emergency department patients with chest pain of uncertain origin. Circulation. 2007; 115:1762–1768.5. Marais BJ, Gie RP, Obihara CC, Hesseling AC, Schaaf HS, Beyers N. Well defined symptoms are of value in the diagnosis of childhood pulmonary tuberculosis. Arch Dis Child. 2005; 90:1162–1165.6. Eslick GD, Talley NJ. Non-cardiac chest pain: predictors of health care seeking, the types of health care professional consulted, work absenteeism and interruption of daily activities. Aliment Pharmacol Ther. 2004; 20:909–915.7. Graves EJ, Gillum BS. Detailed diagnoses and procedures, National Hospital Discharge Survey, 1995. Vital Health Stat 13. 1997; (130):1–146.8. Chapman SJ, Cookson WO, Musk AW, Lee YC. Benign asbestos pleural diseases. Curr Opin Pulm Med. 2003; 9:266–271.9. Currie GP, Watt SJ, Maskell NA. An overview of how asbestos exposure affects the lung. BMJ. 2009; 339:b3209.10. Yates DH, Browne K, Stidolph PN, Neville E. Asbestos-related bilateral diffuse pleural thickening: natural history of radiographic and lung function abnormalities. Am J Respir Crit Care Med. 1996; 153:301–306.11. Kim HY, Song KS, Lee HJ, Lee JS, Lim TH. Parietal pleura and extrapleural space in chronic tuberculous empyema: CT-pathologic correlation. J Comput Assist Tomogr. 2001; 25:9–15.12. Waite RJ, Carbonneau RJ, Balikian JP, Umali CB, Pezzella AT, Nash G. Parietal pleural changes in empyema: appearances at CT. Radiology. 1990; 175:145–150.13. Al-Ghanem S, Al-Jahdali H, Bamefleh H, Khan AN. Bronchiolitis obliterans organizing pneumonia: pathogenesis, clinical features, imaging and therapy review. Ann Thorac Med. 2008; 3:67–75.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pulmonary paragonimiasis: CT findings
- The Diagnostic Significance of 67 Gallium Lung Scan and High Resolution Computed Tomography in Patients with Pulmonary Tuberculosis
- Chest CT finding of Endobronchial Tuberculosis Patients
- Chest Wall Tuberculosis: CT Findings in 14 Patients
- A Study on the Case Rate of Chest Tuberculosis in Female Infertility
