Morphometric Study of Hypoglossal Nerve and Facial Nerve on the Submandibular Region in Korean
- Affiliations
-
- 1Department of Neurosurgery, College of Medicine, Soonchunhyang University, Bucheon, Korea.
- 2Department of Neurosurgery, College of Medicine, Soonchunhyang University, Cheonan, Korea.
- 3Department of Neurosurgery, College of Medicine, Soonchunhyang University, Gumi, Korea.
- 4Department of Neurosurgery, College of Medicine, Soonchunhyang University, Seoul, Korea. j7chang@schmc.ac.kr
- KMID: 2066922
- DOI: http://doi.org/10.3340/jkns.2012.51.5.253
Abstract
OBJECTIVE
This study was performed to determine the anatomical landmarks and optimal dissection points of the facial nerve (FN) and the hypoglossal nerve (HGN) in the submandibular region to provide guidance for hypoglossal-facial nerve anastomosis (HFNA).
METHODS
Twenty-nine specimens were obtained from 15 formalin-fixed adult cadavers. Distances were measured based on the mastoid process tip (MPT), common carotid artery bifurcation (CCAB), and the digastric muscle posterior belly (DMPB).
RESULTS
The shortest distance from the MPT to the stylomastoid foramen was 14.1+/-2.9 mm. The distance from the MPT to the FN origin was 8.6+/-2.8 mm anteriorly and 5.9+/-2.8 mm superiorly. The distance from the CCAB to the crossing point of the HGN and the internal carotid artery was 18.5+/-6.7 mm, and that to the crossing point of the HGN and the external carotid artery was 15.1+/-5.7 mm. The distance from the CCAB to the HGN bifurcation was 26.6+/-7.5 mm. The distance from the digastric groove to the HGN, which was found under the DMPB, was about 35.8+/-5.7 mm. The distance from the digastric groove to the HGN, which was found under the DMPB, corresponded to about 65.5% of the whole length of the DMPB.
CONCLUSION
This study provides useful information regarding the morphometric anatomy of the submandibular region, and the presented morphological data on the nerves and surrounding structures will aid in understanding the anatomical structures more accurately to prevent complications of HFNA.
MeSH Terms
Figure
-
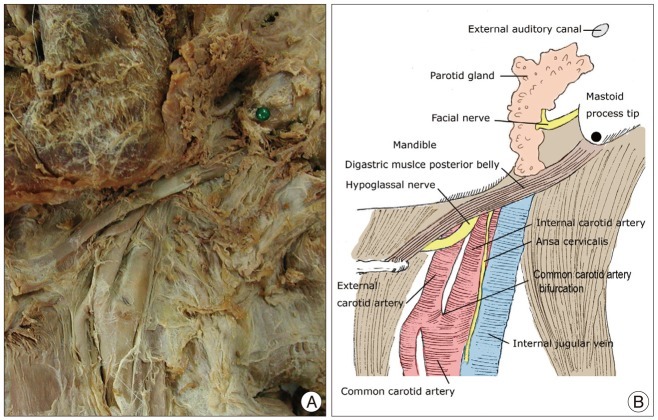
Fig. 1 Neurovascular structures of the submandibular area. A : Photograph showing cadaveric dissection of the submandibular region. Most of the facial nerve (FN) trunk are found in the ventral portion of the mastoid process tip (MPT). Dissection of the FN proximally in the posterior parotid gland (PG) exposed the distal FN trunk and pes anserinus, which is the ramification point of the FN trunk in the PG. B : Schematic representation. Anatomical landmarks are MPT, DMPB, and common carotid artery bifurcation. DMPB : digastric muscle posterior belly.

Fig. 2 Measurements of the distance from the mastoid process tip (MPT) to the stylomastoid foramen (SMF). A : Photograph showing cadaveric dissection of the submandibular region. B : Schematic representation. (A) The shortest distance between the two points. (B) Horizontal distance between the MPT and the SMF. (C) Vertical distance between the SMF and the MPT.
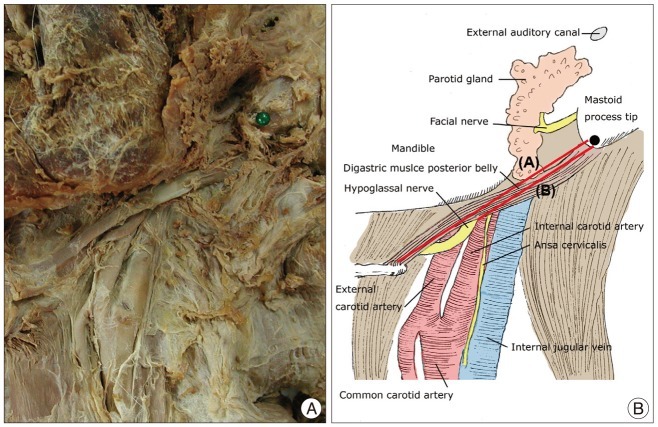
Fig. 3 The digastric muscle posterior belly (DMPB) and hypoglossal nerve (HGN). A : Photograph showing cadaveric dissection of the submandibular region. B : Schematic representation. (A) Whole length of the DMPB. (B) Distance from the DMPB origin to the crossover point of the DMPB inferior border and HGN.
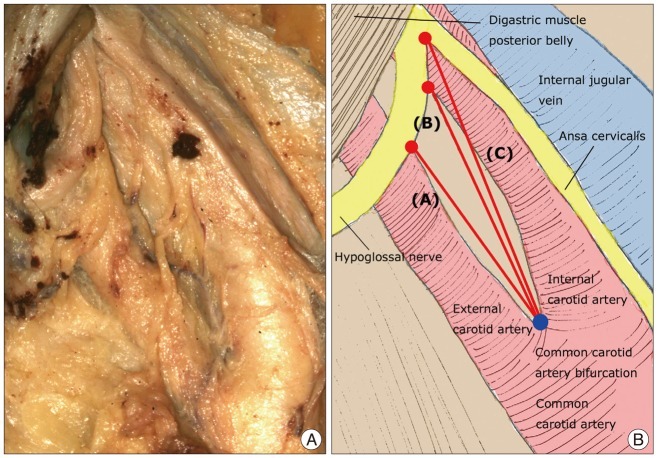
Fig. 4 Relationship between the hypoglossal nerve (HGN) and the carotid artery. A : Photograph showing cadaveric dissection of the submandibular region. B : Schematic representation. (A) Distance from the common carotid artery bifurcation (CCAB) to the crossover point between the external carotid artery and the HGN. (B) Distance from the CCAB to the crossover point between the internal carotid artery and the HGN. (C) Distance from the CCAB to the HGN bifurcation.
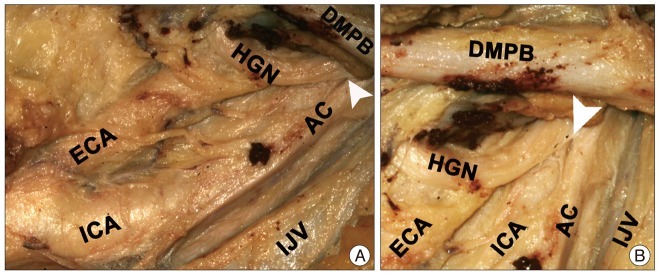
Fig. 5 Photographs showing the relationships among the DMPB, HGN, carotid vessels, and IJV. A : The HGN, neck vessels, and DMPB. B : Magnified view. The white arrow indicates the HGNB. The HGN is located between the ICA and the IJV. It runs parallel to the ICA, gives rise to (white arrow) branches with the ansa cervicalis and crosses the ICA. Separate branches of HGN were found between the DMPB and the CCAB. CCAB : common carotid artery bifurcation, ICA : internal carotid artery, ECA : external carotid artery, DMPB : digastric muscle posterior belly, HGN : hypoglossal nerve, HGNB : hypoglossal nerve bifurcation, AC : ansa cervicalis, IJV : internal jugular vein.
Reference
-
1. Arai H, Sato K, Yanai A. Hemihypoglossal-facial nerve anastomosis in treating unilateral facial palsy after acoustic neurinoma resection. J Neurosurg. 1995; 82:51–54. PMID: 7815134.
Article2. Asaoka K, Sawamura Y. Hypoglossal-facial nerve side-to-end anastomosis. J Neurosurg. 1999; 91:163–164. PMID: 10389900.3. Asaoka K, Sawamura Y, Nagashima M, Fukushima T. Surgical anatomy for direct hypoglossal-facial nerve side-to-end "anastomosis". J Neurosurg. 1999; 91:268–275. PMID: 10433315.
Article4. Cummings C, Fredrickson J, Harker L, Krause C, Richardson M, Schuller D. Hurley R, editor. Otolaryngology head & neck surgery in Hurley R. Otolaryngology Head & Neck Surgery. 1998. Vol 3:ed 3. St. Louis: Mosby-Year Book Inc.;p. 1673–1685.5. Cusimano MD, Sekhar L. Partial hypoglossal to facial nerve anastomosis for reinnervation of the paralyzed face in patients with lower cranial nerve palsies : technical note. Neurosurgery. 1994; 35:532–533. discussion 533-534. PMID: 7800149.
Article6. Decontee J, Joel C, John R. Images from headache : intracranial hypotension complicating Marfan's syndrome. Headache. 2009; 49:1534–1535. PMID: 19912348.
Article7. Ellis E, Zide M. Surgical Approaches to the Facial Skeleton : Surgical Approaches to the Facial Skeleton. 2006. ed 2. Philadelphia: Lippincott Williams & Wilkins;p. 169–189.8. Gordon N. Spontaneous intracranial hypotension. Dev Med Child Neurol. 2009; 51:932–935. PMID: 19909307.
Article9. Halaç M, Albayram S, Ceyhan E, Ozer H, Dogan I, Sager S, et al. Is early bladder activity in radionuclide cisternography an indirect sign of spontaneous intracranial hypotension or sequence of lumbar puncture? Clin Nucl Med. 2007; 32:850–853. PMID: 18075418.
Article10. Kurbanyan K, Lessell S. Intracranial hypotension and abducens palsy following upper spinal manipulation. Br J Ophthalmol. 2008; 92:153–155. PMID: 18156388.
Article11. Lad SP, Li G, Lin SC, Henderson JM. Intracranial hypotension from intrathecal baclofen pump insertion. A case report and review of the literature. Stereotact Funct Neurosurg. 2008; 86:75–79. PMID: 18073519.
Article12. Malone B, Maisel RH. Chapter 2. Anatomy of the facial nerve. Am J Otol. 1988; 9:494–504. PMID: 3232722.13. Martins RS, Socolovsky M, Siqueira MG, Campero A. Hemihypoglossal-facial neurorrhaphy after mastoid dissection of the facial nerve : results in 24 patients and comparison with the classic technique. Neurosurgery. 2008; 63:310–316. discussion 317. PMID: 18797361.14. May M, Sobol SM, Mester SJ. Hypoglossal-facial nerve interpositional-jump graft for facial reanimation without tongue atrophy. Otolaryngol Head Neck Surg. 1991; 104:818–825. PMID: 1908974.
Article15. Rebol J, Milojković V, Didanovic V. Side-to-end hypoglossal-facial anastomosis via transposition of the intratemporal facial nerve. Acta Neurochir (Wien). 2006; 148:653–657. discussion 657. PMID: 16493524.
Article16. Salame K, Ouaknine GE, Arensburg B, Rochkind S. Microsurgical anatomy of the facial nerve trunk. Clin Anat. 2002; 15:93–99. PMID: 11877786.
Article17. Sawamura Y, Abe H. Hypoglossal-facial nerve side-to-end anastomosis for preservation of hypoglossal function : results of delayed treatment with a new technique. J Neurosurg. 1997; 86:203–206. PMID: 9010420.
Article18. Schievink WI, Maya MM. Cerebral venous thrombosis in spontaneous intracranial hypotension. Headache. 2008; 48:1511–1519. PMID: 19076649.
Article19. Schievink WI, Maya MM, Moser F, Tourje J, Torbati S. Frequency of spontaneous intracranial hypotension in the emergency department. J Headache Pain. 2007; 8:325–328. PMID: 18071632.
Article20. Sekhar LN, Schramm VL Jr, Jones NF, Yonas H, Horton J, Latchaw RE, et al. Operative exposure and management of the petrous and upper cervical internal carotid artery. Neurosurgery. 1986; 19:967–982. PMID: 3808244.
Article21. Takeuchi S, Takasato Y, Masaoka H, Hayakawa T, Otani N, Yoshino Y, et al. Spontaneous intracranial hypotension associated with dural sinus thrombosis. . Neurol Med Chir (Tokyo). 2007; 47:555–558. PMID: 18159140.
Article22. Uysal S, Albayram S, Ercan TE. Spontaneous intracranial hypotension : a case report. J Child Neurol. 2008; 23:1312–1315. PMID: 18984842.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Hypoglossal Neurilemmoma in the Submandibular Space
- Delayed Isolated Hypoglossal Nerve Palsy after Submandibular Gland Surgery
- Idiopathic Isolated Hypoglossal Nerve Palsy After Upper Respiratory Infection
- A Case of Facial-Hypoglossal Anastomosis
- Two Cases of Hypoglossal Neurilemmoma in the Submandibular Space
