J Korean Endocr Soc.
2007 Aug;22(4):266-271. 10.3803/jkes.2007.22.4.266.
A Case of Turner's Syndrome with Transient Hypopituitarism
- Affiliations
-
- 1Department of Internal Medicine, Yonsei Universitiy College of Medicine.
- KMID: 2063536
- DOI: http://doi.org/10.3803/jkes.2007.22.4.266
Abstract
- Turner's syndrome is characterized by short stature and gonadal dysgenesis, and it is often associated with various systemic manifestations, such as cardiovascular, renal, thyroidal, gastrointestinal, and musculoskeletal disorders. Though very rare, it can also be accompanied by hypopituitarism. It is important to give a meticulous medical attention to short females with gonadal dysgenesis so that neither disease is neglected or gets delayed diagnosis. In this case, Turner's syndrome and hypopituitarism were diagnosed almost simultaneously, but hypopiuitarism was transient, and the normal pituitary function was recovered spontaneously without any treatment. Initial sella MRI showed mild congenital hypoplastic hypopituitarism, and combined pituitary function test was compatible with hypopituitarism, but after 5 years, though growth hormone deficiency was still present, otherwise normal pituitary function was noted without any change in MRI. Herein, we are reporting a case of Turner's syndrome with transient idiopathic hypopituitarism with the review of literature.
MeSH Terms
Figure
-
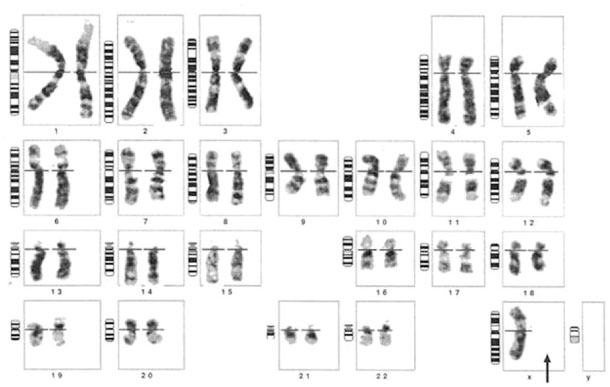
Fig. 1 The patient has karyotype of 45,X/46,XX.
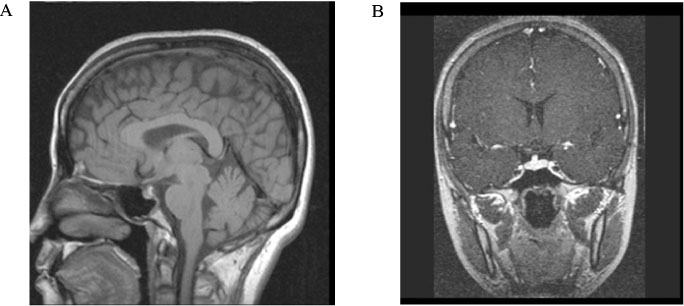
Fig. 2 Sella dynamic MRI (2001.4.8). Mild, diffuse shrinkage of pituitary gland with slightly upward displacement and reduced size of neurohypophysis is seen, compatible with congenital hypoplasitc hypopituitarism.
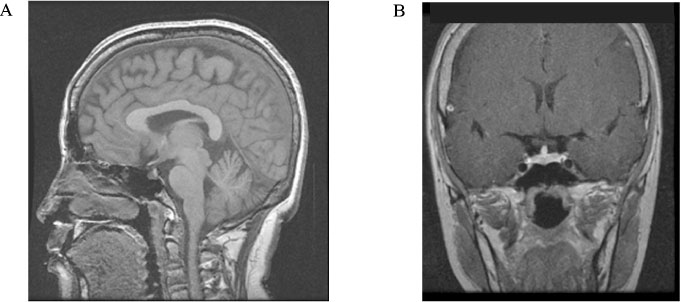
Fig. 3 Sella dynamic MRI (2006.10.13). No remarkable interval change of pituitary gland size and shape on this study. Mild hypoplastic pituitary gland is suggested.
Reference
-
1. Saenger P. Turner's syndrome. N Engl J Med. 1996. 335:1749–1754.2. Cracowski JL, Vanzetto G, Douchin S, Atger O, Bost M, Machecourt J. Myocardial infarction and Turner's syndrome. Clin Cardiol. 1999. 22:245–247.3. Nishi N, Sakano T, Hyodo S, Masuda H, Kitamura Y, Shindo H, Sakoda H, Uozumi T, Usui T. Pituitary abnormalities detected by high resolution computed tomography with thin slices in primary hypopituitarism and Turner's syndrome. Eur J Pediatr. 1984. 142:25–28.4. Samaan NA, Stepanas AV, Danziger J, Trujillo J. Reactive pituitary abnormalities in patients with Klinefelters and Turner's syndromes. Arch Intern Med. 1979. 139:198–201.5. Kim HS, Byun JW, Yoon DS, Kim DH, Seo BK, Shin YK, Chung CH. A case of Turner syndrome associated with autoimmune thyroiditis and empty sella. J Kor Soc Endocrinol. 1996. 11:114–118.6. Gallicchio CT, Alves ST, Ramos HI, Llerena JC, Guimaraes MM. Association of Turner's syndrome and hypopituitarism: a patient report. J Pediatr Endocrinol Metab. 2003. 16:901–905.7. Efstathiadou Z, Tsatsoulis A. Turner's syndrome with concomitant hypopituitarism. Hum Reproduction. 2000. 15:2388–2389.8. Kim MN, Han HO, Kim SW, Yang IM, Kim JW, Kim YS, Kim KW, Choi YK. A case of low grade Turners syndrome. Kor J Intern Med. 1988. 35:564–568.9. Lomna-Bogdanov E, Bolanowski M, Slezak R, Sokolska V, Palczyinski B, Spring A, Demissie M. Familial hypopituitarism associated with mosaic form of Turner syndrome. Gynecol Endocrinol. 2005. 20:22–25.10. Simpson JL. Gonadal dysgenesis and abnormal human sex chromosomes; current status of phenotypic-karyotypic correlations. Birth Defects Orig Artic Ser. 1975. 11:23–59.11. Pasquino AM, Passeri F, Pucarelli I, Segni M, Municchi G. Spontaneous pubertal development in Turner's syndrome. Italian Study Group for Turner's Syndrome. J Clin Endocrinol Metab. 1997. 82:1810–1813.12. Elsheikh M, Dunger DB, Conway GS, Wass JA. Turner's Syndrome in Adulthood. Endocr Rev. 2002. 23:120–140.13. Ranke MB, Saenger P. Turner's syndrome. Lancet. 2001. 358:309–314.14. McDonough PG, Tho PT. Gonadal dysgenesis with atypical bleeding, functional cyst in rudimentary streak gonads. Am J Obstet Gynecol. 1974. 119:565–567.15. Garel C, Leger J. Contribution of magnetic resonance imaging in non-tumoral hypopituitarism in children. Horm Res. 2007. 67:194–202.16. Silver HS, Morris LR. Hypopituitarism secondary to cavernous sinus thrombosis. South Med J. 1983. 76:642–646.17. Martin FIR. Spontaneous cure of hypopituitarism. Endocrinologist. 1994. 4:184–188.18. Tan GH, Young WF Jr. Transient hypopituitarism. Endocr Pract. 1995. 1:320–322.19. Eiholzer U, Zachmann M, Gnehm HE, Prader A. Recovery from post-traumatic anterior pituitary insufficiency. Eur J Pediatr. 1986. 145:128–130.20. Zadik Z, Landau H, Chen M, Altman Y, Lieberman E. Assessment of growth hormone (GH) axis in Turner's syndrome using 24-hour integrated concentrations of GH, insulin-like growth factor-I, plasma GH-binding activity, GH binding to IM9 cells, and GH response to pharmacological stimulation. J Clin Endocrinol Metab. 1992. 75:412–416.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of Prune Belly syndrome associated with Turner syndrome
- A case of hypomelanosis of Ito accompanying Turner syndrome
- A case of isochromosome Xq Turner syndrome associated with metabolic syndrome and autoimmune thyroiditis
- A Case of Down-Turner Syndrome
- A Case of Turner Syndrome Presenting as Aneurysmal Subarachnoid Hemorrhage
