Frozen Section Biopsy to Evaluation of Obscure Lateral Resection Margins during Gastric Endoscopic Submucosal Dissection for Early Gastric Cancer
- Affiliations
-
- 1Institute for Digestive Research, Digestive Disease Center, Soonchunhyang University College of Medicine, Seoul, Korea. schcjy@schmc.ac.kr
- 2Department of Pathology, Soonchunhyang University College of Medicine, Seoul, Korea.
- 3Institute for Statistics and Education Consulting, StatEdu, Seoul, Korea.
- KMID: 2055512
- DOI: http://doi.org/10.5230/jgc.2011.11.3.155
Abstract
- PURPOSE
To determine the diagnostic utility of a frozen section biopsy in patients undergoing endoscopic submucosal dissection (ESD) for early gastric neoplasms with obscure margins even with chromoendoscopy using acetic acid and indigo carmine (AI chromoendoscopy).
MATERIALS AND METHODS
The lateral spread of early gastric neoplasms was unclear even following AI chromoendoscopy in 38 patients who underwent ESD between June 2007 and May 2011. Frozen section biopsies were obtained by agreement of the degree of lateral spread between two endoscopists. Thus, frozen section biopsies were obtained from 23 patients (FBx group) and not in the other 15 patients (AI group).
RESULTS
No significant differences were observed for size, histology, invasive depth, and location of lesions between the AI and FBx groups. No false positive or false negative results were observed in the frozen section diagnoses. Adenocarcinoma was revealed in three patients and tubular adenoma in one, thereby changing the delineation of lesion extent and achieving free lateral margins. The rates of free lateral resection margins and curative resection were significantly higher in the FBx group than those in the AI group.
CONCLUSIONS
Frozen section biopsy can help endoscopists perform more safe and accurate ESD in patients with early gastric neoplasm.
Keyword
MeSH Terms
Figure
-
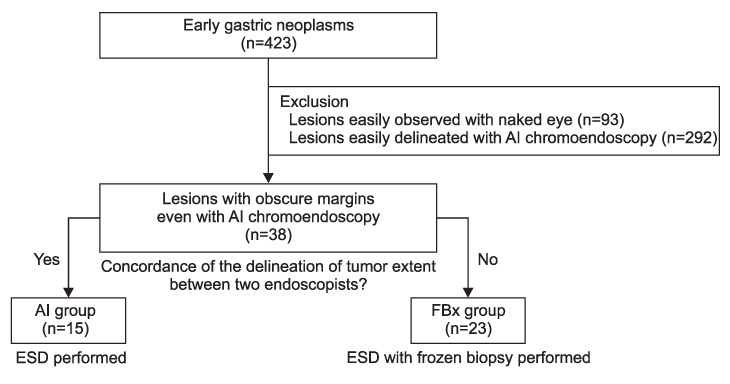
Fig. 1 Study design. ESD = endoscopic submucosal dissection.

Fig. 2 A representative case of gastric tubular adenoma in which frozen section biopsy was performed before endoscopic submucosal dissection. (A) A slightly elevated gastric lesion with unclear margin in white light was noticed in the lower third stomach. (B) The lateral spread of the lesion was still obscure despite of chromoendoscopy using acetic acid and indigo carmine. (C) A frozen section biopsy was performed 5mm distal to expected lateral extent of the lesion, which was selected by the experienced endoscopist (Cho JY), because the lesions showed disconcordance in the assessment of lateral spread between two endoscopists. (D) The outer surface of the specimen was marked with special ink (the Davidson Marking System® Bradely product Inc.) to provide a pathologist (Jin SY) orientation of specimens. (E) We marked several spots near the site, where frozen section biopsy was done, because frozen section revealed chronic gastritis with intestinal metaplasia. (F) En bloc resection of the lesion was performed. (G) A site of frozen section biopsy was observed in the resected specimen. (H) Pathologic mapping showed curatively resected tubular adenoma (The orange line indicated the lesion, tubular adenoma).
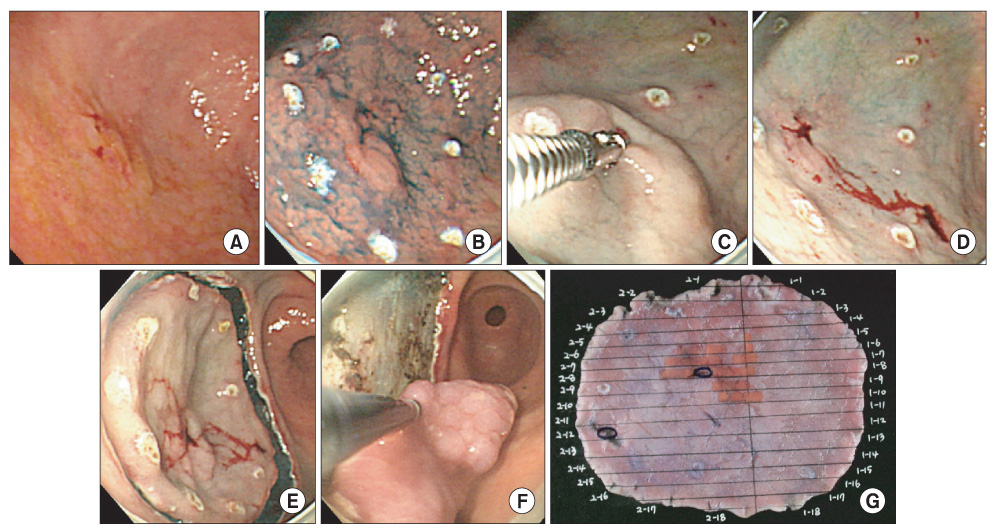
Fig. 3 A representative case of adenocarcinoma in which frozen section result revealed adenocarcinoma, thus achieved free lateral margin. (A) A slightly elevated gastric lesion with unclear margin in white light was noticed in antrum. (B) The lateral spread of the lesion was still obscure despite of chromoendoscopy using acetic acid and indigo carmine. (C) A frozen section biopsy was performed 3mm away from the expected lateral extent of the lesion, which was selected by the experienced endoscopist (Cho JY), because the lesions showed disconcordance in the assessment of lateral spread between two endoscopists. (D) We marked several spots about 1 cm away from the site, where frozen section biopsy was done, because frozen section revealed adenocarcinoma, well differenciated. The second biopsy revealed chronic gastritis with focal intestinal metaplasia. (E) A circumferential mucosal incision was made around the lesion including frozen section biopsy sites. (F) En bloc resection of the lesion was performed. (G) Pathologic mapping showed curatively resected adenocarcinoma (The orange line indicated the lesion - adenocarcinoma. And blue circles indicated frozen section biopsy sites).
Reference
-
1. Nakayoshi T, Tajiri H, Matsuda K, Kaise M, Ikegami M, Sasaki H. Magnifying endoscopy combined with narrow band imaging system for early gastric cancer: correlation of vascular pattern with histopathology (including video). Endoscopy. 2004. 36:1080–1084.
Article2. Tamai N, Kaise M, Nakayoshi T, Katoh M, Sumiyama K, Gohda K, et al. Clinical and endoscopic characterization of depressed gastric adenoma. Endoscopy. 2006. 38:391–394.
Article3. Otsuka Y, Niwa Y, Ohmiya N, Ando N, Ohashi A, Hirooka Y, et al. Usefulness of magnifying endoscopy in the diagnosis of early gastric cancer. Endoscopy. 2004. 36:165–169.
Article4. Yao K, Anagnostopoulos GK, Ragunath K. Magnifying endoscopy for diagnosing and delineating early gastric cancer. Endoscopy. 2009. 41:462–467.
Article5. Yagi K, Aruga Y, Nakamura A, Sekine A, Umezu H. The study of dynamic chemical magnifying endoscopy in gastric neoplasia. Gastrointest Endosc. 2005. 62:963–969.
Article6. Sakai Y, Eto R, Kasanuki J, Kondo F, Kato K, Arai M, et al. Chromoendoscopy with indigo carmine dye added to acetic acid in the diagnosis of gastric neoplasia: a prospective comparative study. Gastrointest Endosc. 2008. 68:635–641.
Article7. Yamashita H, Kitayama J, Ishigami H, Yamada J, Miyato H, Kaisaki S, et al. Endoscopic instillation of indigo carmine dye with acetic acid enables the visualization of distinct margin of superficial gastric lesion; Usefulness in endoscopic treatment and diagnosis of gastric cancer. Dig Liver Dis. 2007. 39:389–391.
Article8. Iizuka T, Kikuchi D, Hoteya S, Yahagi N. The acetic acid + indigocarmine method in the delineation of gastric cancer. J Gastroenterol Hepatol. 2008. 23:1358–1361.
Article9. Kawahara Y, Takenaka R, Okada H, Kawano S, Inoue M, Tsuzuki T, et al. Novel chromoendoscopic method using an acetic acid-indigocarmine mixture for diagnostic accuracy in delineating the margin of early gastric cancers. Dig Endosc. 2009. 21:14–19.
Article10. Japanese Gastric Cancer Association. Japanese Classification of Gastric Carcinoma - 2nd English Edition -. Gastric Cancer. 1998. 1:10–24.11. Kuznetsov K, Lambert R, Rey JF. Narrow-band imaging: potential and limitations. Endoscopy. 2006. 38:76–81.
Article12. Kaufman Z, Lew S, Griffel B, Dinbar A. Frozen-section diagnosis in surgical pathology. A prospective analysis of 526 frozen sections. Cancer. 1986. 57:377–379.
Article13. Howanitz PJ, Hoffman GG, Zarbo RJ. The accuracy of frozen-section diagnoses in 34 hospitals. Arch Pathol Lab Med. 1990. 114:355–359.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Treatment for Early Gastric Cancer
- Endoscopic Resection of Early Gastric Cancer
- Endoscopic Resection of Early Gastric Cancer in Korea: Recent Results and Future Directions
- Discrepancy between Clinical and Final Pathological Evaluation Findings in Early Gastric Cancer Patients Treated with Endoscopic Submucosal Dissection
- Endoscopic treatment for early gastric cancer
