Arthroscopic Treatment for External Snapping Hip
- Affiliations
-
- 1Department of Orthopaedic Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. orthoyoon@amc.seoul.kr
- 2Department of Orthopedic Surgery, Joint and Spine Center, SMG-SNU Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2054181
- DOI: http://doi.org/10.5371/hp.2014.26.3.173
Abstract
- PURPOSE
The purpose of this study was to evaluate the clinical outcome of arthroscopic treatment for recalcitrant external snapping hip.
MATERIALS AND METHODS
Between September 2011 and June 2013, we evaluated 7 patients (10 cases) with snapping hip who were refractory to conservative treatments for at least 3 months. Two patients (4 cases) were impossible to adduct both knees in 90degreesof hip flexion. Surgery was done in lateral decubitus position, under spinal anesthesia. We made 2 arthroscopic portals to operate the patients, and used cross-cutting with flap resection technique to treat the lesion. We performed additional gluteal sling release in those 2 patients (4 cases) with adduction difficulty. Average follow-up length was 19 months (range, 12-33 months). Clinical improvement was evaluated with visual analog scale (VAS), modified Harris hip score (mHHS), and also investigated for presence of limping or other complications as well.
RESULTS
The VAS decreased from 6.8 (range, 6-9) preoperatively to 0.2 (range, 0-2) postoperatively, and the mHHS improved from 68.2 to 94.8 after surgery. None of the patients complained of post-operative wound problem or surgical complications.
CONCLUSION
The clinical outcome of arthroscopic treatment for recalcitrant external snapping hip was encouraging and all patients were also satisfied with the cosmetic results.
MeSH Terms
Figure
-

Fig. 1 Surgeon's view of the surgical field (left hip). The patient lies in lateral decubitus position and head is to the right. Greater trochanter is delineated on the skin as a curve and two portals were used.
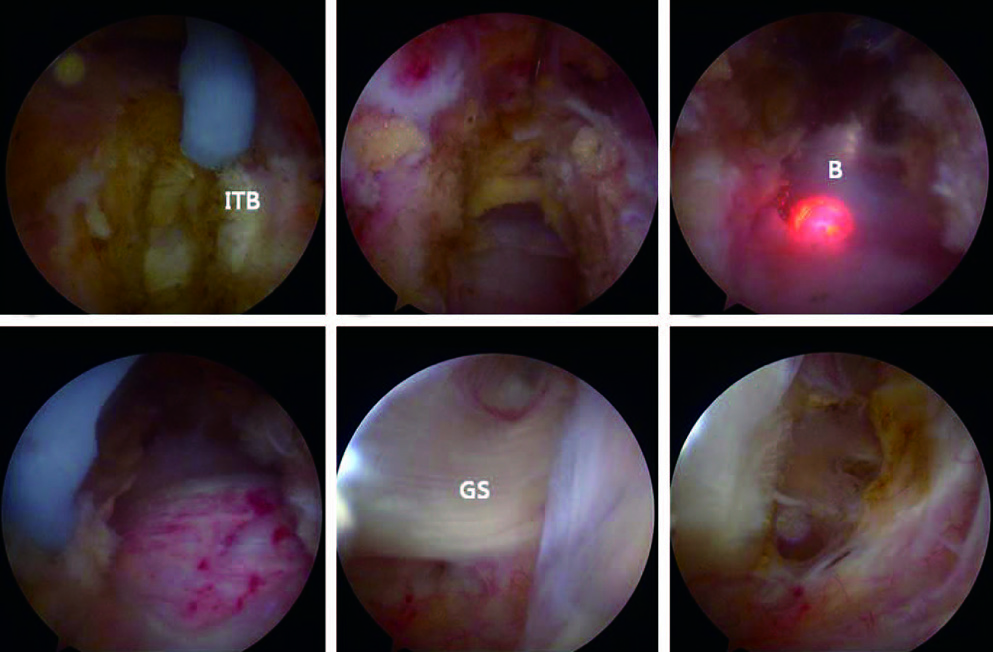
Fig. 2 Arthroscopic images of left hip of 33-year old female patient. (A) Longitudinal cut is started on the iliotibial band (ITB) distal to the greater trochanter and directed proximally. (B) The final diamondshaped defect of the ITB. (C) Trochanteric bursa is resected through the defect using a shaver and a radiofrequency ablator. (D) Greater trochanter can be observed through the defect after bursectomy. (E) Gluteal sling of the gluteus maximus muscle, inserting to linea aspera. (F) Gluteal sling can be easily and safely released using a flexible radiofrequency ablator.
Reference
-
1. Polesello GC, Queiroz MC, Domb BG, Ono NK, Honda EK. Surgical technique: Endoscopic gluteus maximus tendon release for external snapping hip syndrome. Clin Orthop Relat Res. 2013; 471:2471–2476.
Article2. Teitz CC, Garrett WE Jr, Miniaci A, Lee MH, Mann RA. Tendon problems in athletic individuals. Instr Course Lect. 1997; 46:569–582.3. Provencher MT, Hofmeister EP, Muldoon MP. The surgical treatment of external coxa saltans (the snapping hip) by Z-plasty of the iliotibial band. Am J Sports Med. 2004; 32:470–476.
Article4. White RA, Hughes MS, Burd T, Hamann J, Allen WC. A new operative approach in the correction of external coxa saltans: the snapping hip. Am J Sports Med. 2004; 32:1504–1508.
Article5. Ilizaliturri VM Jr, Martinez-Escalante FA, Chaidez PA, Camacho-Galindo J. Endoscopic iliotibial band release for external snapping hip syndrome. Arthroscopy. 2006; 22:505–510.
Article6. Brignall CG, Stainsby GD. The snapping hip. Treatment by Z-plasty. J Bone Joint Surg Br. 1991; 73:253–254.
Article7. Zoltan DJ, Clancy WG Jr, Keene JS. A new operative approach to snapping hip and refractory trochanteric bursitis in athletes. Am J Sports Med. 1986; 14:201–204.
Article8. Ilizaliturri VM Jr, Camacho-Galindo J. Endoscopic treatment of snapping hips, iliotibial band, and iliopsoas tendon. Sports Med Arthrosc. 2010; 18:120–127.
Article9. Nam KW, Yoo JJ, Koo KH, Yoon KS, Kim HJ. A modified Z-plasty technique for severe tightness of the gluteus maximus. Scand J Med Sci Sports. 2011; 21:85–89.
Article10. Jacobsen JS, Søballe K, Ulrich-Vinther M. Eccentric hip abductor weakness in patients with symptomatic external snapping hip. Scand J Med Sci Sports. 2012; 22:e140–e146.
Article11. Brignall CG, Brown RM, Stainsby GD. Fibrosis of the gluteus maximus as a cause of snapping hip. A case report. J Bone Joint Surg Am. 1993; 75:909–910.
Article12. Allen WC, Cope R. Coxa saltans: The snapping hip revisited. J Am Acad Orthop Surg. 1995; 3:303–308.
Article13. Yoon TR, Park KS, Diwanji SR, Seo CY, Seon JK. Clinical results of multiple fibrous band release for the external snapping hip. J Orthop Sci. 2009; 14:405–409.
Article14. Jacobson T, Allen WC. Surgical correction of the snapping iliopsoas tendon. Am J Sports Med. 1990; 18:470–474.
Article15. Féry A, Sommelet J. The snapping hip. Late results of 24 surgical cases. Int Orthop. 1988; 12:277–282.16. Faraj AA, Moulton A, Sirivastava VM. Snapping iliotibial band. Report of ten cases and review of the literature. Acta Orthop Belg. 2001; 67:19–23.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Arthroscopic Resection of Osteochondroma of Hip Joint Associated with Internal Snapping: A Case Report
- Snapping Knee caused by the Gracilis and Semitendinosus tendon
- Osteochondroma Arising from Anterior Inferior Iliac Spine as a Cause of Snapping Hip
- Arthroscopic Treatment of Symptomatic Internal Snapping Hip with Combined Pathologies
- External Snapping Hip Treated by Effective Designed N-plasty of the Iliotibial Band
