Metastatic Pulmonary Mucoepidermoid Carcinoma with Fulminant Clinical Course
- Affiliations
-
- 1Department of Internal Medicine, KEPCO Medical Center, Seoul, Korea. humanmd04@hanmail.net
- 2Department of Pathology, KEPCO Medical Center, Seoul, Korea.
- 3Division of Respiratory and Critical Care Medicine, Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 2052787
- DOI: http://doi.org/10.12771/emj.2015.38.2.85
Abstract
- Pulmonary mucoepidermoid carcinoma (MEC) is a rare form of lung cancer that originates from submucosal glands of tracheobronchial tree. Unlike low-grade tumor with benign nature, high-grade case is even rarer and has aggressive clinical features with no definite treatment option. Here, we report a case of high-grade pulmonary MEC with fulminant clinical course. A 74-year-old man presented with cough, sputum and mental change. Chest imaging showed massive mediastinal lymphadenopathy with obstructive pneumonia, and multiple metastases in lung and adrenal gland. Bronchoscopy showed polypoid masses obstructing right main bronchus and bronchus intermedius. Histopathology revealed a mixture of glandular structure lined with mucussecreting cells and nests of squamoid cells with nuclear atypia and pleomorphism, which is compatible with high-grade MEC. We intensively treated the patient with combination antibiotics and ventilator care. However, the patient did not respond to the treatment and rapidly deteriorated, and finally expired a month after diagnosis.
Keyword
MeSH Terms
Figure
-

Fig. 1 Chest radiography at presentation. It shows increased opacity at right lower lung field and hyperlucent left lung, suggestive of collapsed right lower lobe.
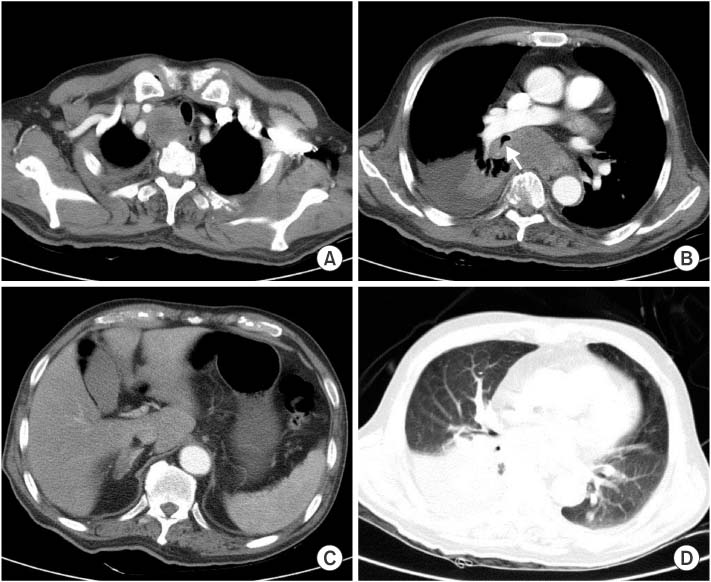
Fig. 2 Chest computed tomography scan. It reveals hugely enlarged upper paratracheal lymph node compressing trachea (A), and subcarinal lymph node and an endobronchial mass arrow associated with atelectasis of right lower lobe and pleural effusion (B). About 2 cm-sized right adrenal mass (C) and a metastatic nodule in left lower lung were also noted (D).

Fig. 3 Bronchoscopic findings. It shows two endobronchial masses arising at right main bronchus and the orifice of right bronchus intermedius. The masses are 1-2 cm-sized, well-circumscribed hypervascular polypoid tumors.
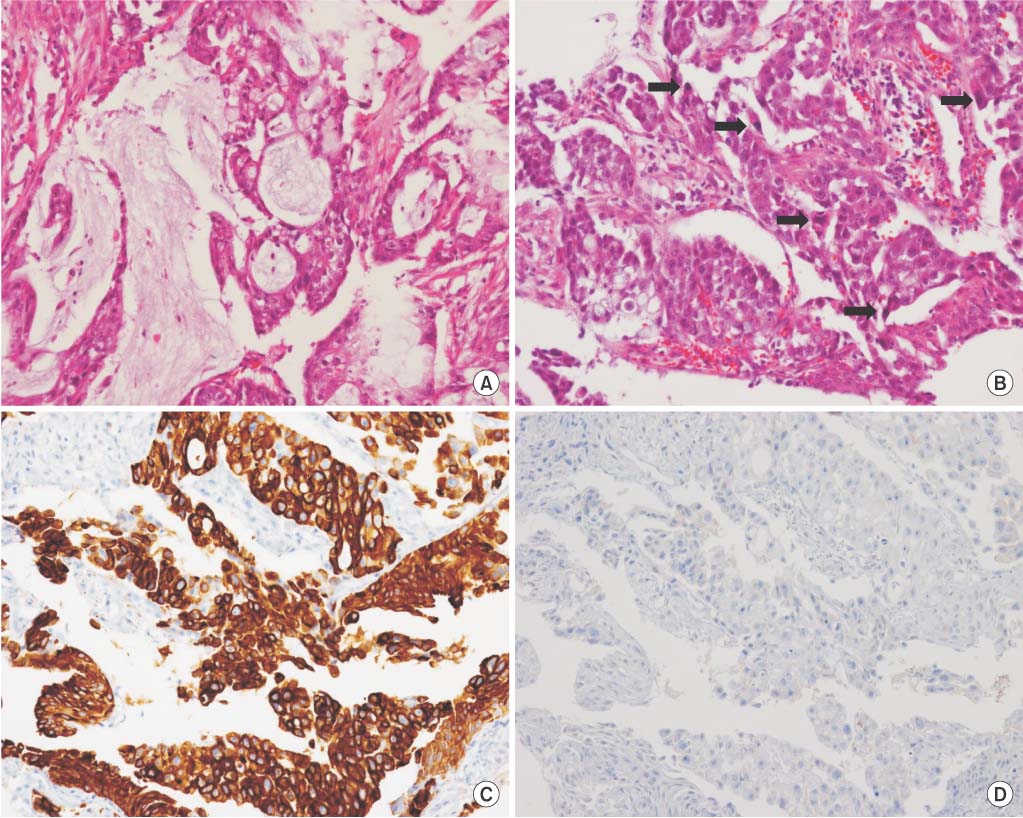
Fig. 4 Histopathologic images. Hematoxylin and eosin staining shows glandular structures with mucus-secreting cells (A), nests of squamoid and intermediated cells (B). Immnuohistochemistry shows positive staining in cytokeratin 7 (C) and negative staining in thyroid transcription factor-1 (D). The nuclei are pleomorphic and show frequent mitosis (arrows), compatible with high-grade mucoepidermoid carcinoma (×200).
Reference
-
1. Miller DL, Allen MS. Rare pulmonary neoplasms. Mayo Clin Proc. 1993; 68:492–498.2. Yousem SA, Hochholzer L. Mucoepidermoid tumors of the lung. Cancer. 1987; 60:1346–1352.3. Seethala RR. An update on grading of salivary gland carcinomas. Head Neck Pathol. 2009; 3:69–77.4. Heitmiller RF, Mathisen DJ, Ferry JA, Mark EJ, Grillo HC. Mucoepidermoid lung tumors. Ann Thorac Surg. 1989; 47:394–399.5. Vadasz P, Egervary M. Mucoepidermoid bronchial tumors: a review of 34 operated cases. Eur J Cardiothorac Surg. 2000; 17:566–569.6. Chin CH, Huang CC, Lin MC, Chao TY, Liu SF. Prognostic factors of tracheobronchial mucoepidermoid carcinoma: 15 years experience. Respirology. 2008; 13:275–280.7. Rossi G, Sartori G, Cavazza A, Tamberi S. Mucoepidermoid carcinoma of the lung, response to EGFR inhibitors, EGFR and KRAS mutations, and differential diagnosis. Lung Cancer. 2009; 63:159–160.8. Goode RK, Auclair PL, Ellis GL. Mucoepidermoid carcinoma of the major salivary glands: clinical and histopathologic analysis of 234 cases with evaluation of grading criteria. Cancer. 1998; 82:1217–1224.9. Song Z, Liu Z, Wang J, Zhu H, Zhang Y. Primary tracheobronchial mucoepidermoid carcinoma: a retrospective study of 32 patients. World J Surg Oncol. 2013; 11:62.10. Ha SY, Han J, Lee JJ, Kim YE, Choi YL, Kim HK. Mucoepidermoid carcinoma of tracheobronchial tree: clinicopathological study of 31 cases. Korean J Pathol. 2011; 45:175–181.11. Han SW, Kim HP, Jeon YK, Oh DY, Lee SH, Kim DW, et al. Mucoepidermoid carcinoma of lung: potential target of EGFRdirected treatment. Lung Cancer. 2008; 61:30–34.12. Lee KW, Chan AB, Lo AW, Lam KC. Erlotinib in metastatic bronchopulmonary mucoepidermoid carcinoma. J Thorac Oncol. 2011; 6:2140–2141.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cytopathology of Metastatic Mucoepidermoid Carcioma of the Lung
- A Case of Mucoepidermoid Carcinoma in Pulmonary Tuberculosis Patient
- A Case of Conjunctival Mucoepidermoid Carcinoma with invioving Cornea
- A Case of Hypertrophic Osteoarthropathy Associated with Lung Metastasis of Parotid Gland Mucoepidermoid Carcinoma
- Mucoepidermoid Carcinoma in The External Auditory Canal: A Case Report
