Atypical Kawasaki Disease Presenting as Acute Kidney Injury in a Patient with Influenza B Virus Infection
- Affiliations
-
- 1Department of Pediatrics, Ewha Womans University School of Medicine, Seoul, Korea. sohn@ewha.ac.kr
- KMID: 2052786
- DOI: http://doi.org/10.12771/emj.2015.38.2.80
Abstract
- Influenza virus infection is a common respiratory disease in children. Renal complications of influenza infection were not commonly encountered until the 2009 H1N1 influenza pandemic, when acute kidney injury (AKI) frequently developed in severely ill patients. Kawasaki disease (KD) is another rare association in pandemic influenza virus infections. There are some reports about KD coincident with influenza A H1N1/09 infection. However, simultaneous AKI and KD in influenza A or B virus infections have never been reported. Herein, we report the first case of influenza B virus infection that initially presented as AKI but was subsequently diagnosed as atypical KD.
MeSH Terms
Figure
-
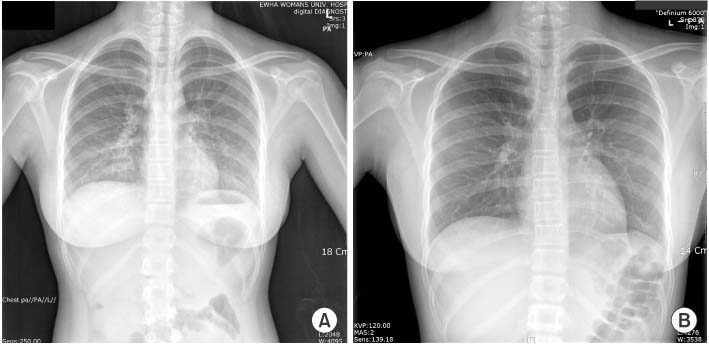
Fig. 1 (A) Initial chest radiograph. It shows hazy increased opacity suggesting pneumonia, and pulmonary edema in both lower lung fields. (B) Repeat chest radiography. It shows no residual lesions in both lungs.
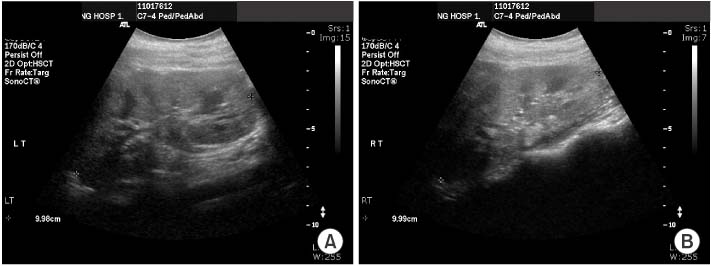
Fig. 2 Renal ultrasonography. (A, B) It shows slightly increased cortical echogenicity of both kidneys, suggestive of renal parenchymal disease.

Fig. 3 Photographs of hand of foot on the 4th hospital day. It shows desquamation and peeling of fingers (A), toes and soles (B).
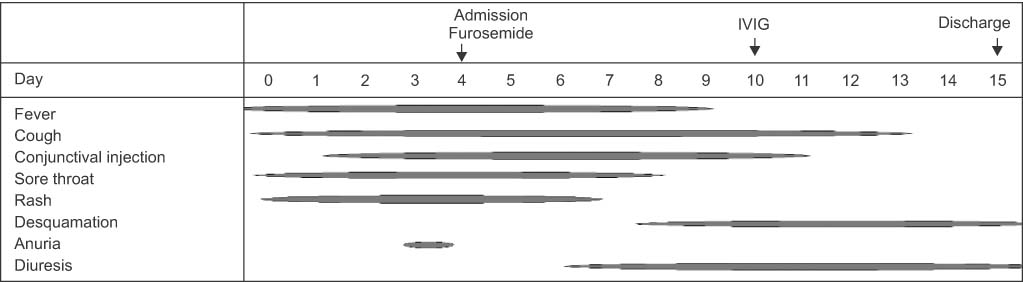
Fig. 4 The clinical course of the patient. The patient was initially diagnosed with influenza B virus infection and acute kidney injury after presenting with fever, cough, conjunctival injection, sore throat and skin rash followed by anuria. Diuresis occurred on the 3rd hospital day. Subsequently, periungual desquamation developed and intravenous immunoglobulin (IVIG) was administered under the diagnosis of Kawasaki disease.

Fig. 5 Serial changes in the estimated glomerular filtration rate (eGFR), serum creatinine (Cr), and albumin (alb) related to the hospital day (HD). A low eGFR and a high Cr at the time of admission were restored to within the normal range during the hospitalization.
Reference
-
1. Jung JY, Park BH, Hong SB, Koh Y, Suh GY, Jeon K, et al. Acute kidney injury in critically ill patients with pandemic influenza A pneumonia 2009 in Korea: a multicenter study. J Crit Care. 2011; 26:577–585.2. Watanabe T. Renal complications of seasonal and pandemic influenza A virus infections. Eur J Pediatr. 2013; 172:15–22.3. Bagshaw SM, Sood MM, Long J, Fowler RA, Adhikari NK. Canadian Critical Care Trials Group H1N1 Collaborative. Acute kidney injury among critically ill patients with pandemic H1N1 influenza A in Canada: cohort study. BMC Nephrol. 2013; 14:123.4. Abe M, Higuchi T, Okada K, Kaizu K, Matsumoto K. Clinical study of influenza-associated rhabdomyolysis with acute renal failure. Clin Nephrol. 2006; 66:166–170.5. Sevignani G, Soares MF, Marques GL, Freitas AK, Gentili A, Chula DC, et al. Acute kidney injury in patients infected by H1N1: clinical histological correlation in a series of cases. J Bras Nefrol. 2013; 35:185–190.6. Brottet E, Vandroux D, Gauzere BA, Antok E, Jaffar-Bandjee MC, Michault A, et al. Influenza season in Réunion dominated by influenza B virus circulation associated with numerous cases of severe disease, France, 2014. Euro Surveill. 2014; 19(39):pii=20916.7. Joshi AV, Jones KD, Buckley AM, Coren ME, Kampmann B. Kawasaki disease coincident with influenza A H1N1/09 infection. Pediatr Int. 2011; 53:e1–e2.8. Kim GB, Park S, Kwon BS, Han JW, Park YW, Hong YM. Evaluation of the temporal association between Kawasaki disease and viral infections in South Korea. Korean Circ J. 2014; 44:250–254.9. Fukushige J, Takahashi N, Ueda Y, Ueda K. Incidence and clinical features of incomplete Kawasaki disease. Acta Paediatr. 1994; 83:1057–1060.10. Hicks RV, Melish ME. Kawasaki syndrome. Pediatr Clin North Am. 1986; 33:1151–1175.11. Salcedo JR, Greenberg L, Kapur S. Renal histology of mucocutaneous lymph node syndrome (Kawasaki disease). Clin Nephrol. 1988; 29:47–51.12. Newburger JW, Takahashi M, Gerber MA, Gewitz MH, Tani LY, Burns JC, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic fever, endocarditis and Kawasaki Disease, council on cardiovascular disease in the young, American heart association. Circulation. 2004; 110:2747–2771.13. Papadodima SA, Sakelliadis EI, Goutas ND, Vlachodimitropoulos DG, Spiliopoulou CA. Atypical kawasaki disease presenting with symptoms from the genitourinary system: an autopsy report. J Trop Pediatr. 2009; 55:55–57.14. Smith LB, Newburger JW, Burns JC. Kawasaki syndrome and the eye. Pediatr Infect Dis J. 1989; 8:116–118.15. Lee H, Kim H, Kim HS, Sohn S. NT-pro BNP:a new diagnostic screening tool for Kawasaki disease. Korean J Pediatr. 2006; 49:539–544.
