Electrolyte Blood Press.
2007 Dec;5(2):126-130. 10.5049/EBP.2007.5.2.126.
Electrolyte and Acid-Base Disturbances Induced by Clacineurin Inhibitors
- Affiliations
-
- 1Department of Internal Medicine, Hanyang University College of Medicine, Seoul, Korea. changhaw@hanyang.ac.kr
- KMID: 2052295
- DOI: http://doi.org/10.5049/EBP.2007.5.2.126
Abstract
- Nephrotoxicity is the most common and clinically significant adverse effect of calcineurin inhibitors. Cyclosporine and tacrolimus nephrotoxicity is manifested by both acute azotemia and chronic progressive renal disease and tubular zdysfunction. An elevation in the plasma potassium concentration due to reduced efficiency of urinary potassium excretion is common in cyclosporine-treated patients; it may be severe and potentially life-threatening with concurrent administration of an angiotensin converting enzyme inhibitor, which diminishes aldosterone release. Tubular injury induced by cyclosporine can also impair acid excretion. This may be presented as a hyperchloremic metabolic acidosis associated with decreased aldosterone activity and suppression of ammonium excretion by hyperkalemia. Some patients treated with cyclosporine develop hypophosphatemia due to urinary phosphate wasting. Renal magnesium wasting is also common presumably due to drug effects on magnesium reabsorption. Hypomagnesemia has also been implicated as a contributor to the nephrotoxicity associated with cyclosporine. Both cyclosporine and tacrolimus are associated with hypercalciuria. Attention must be paid to drug dose, side effects, and drug interactions to minimize toxicity and maximize efficacy.
MeSH Terms
Figure
-
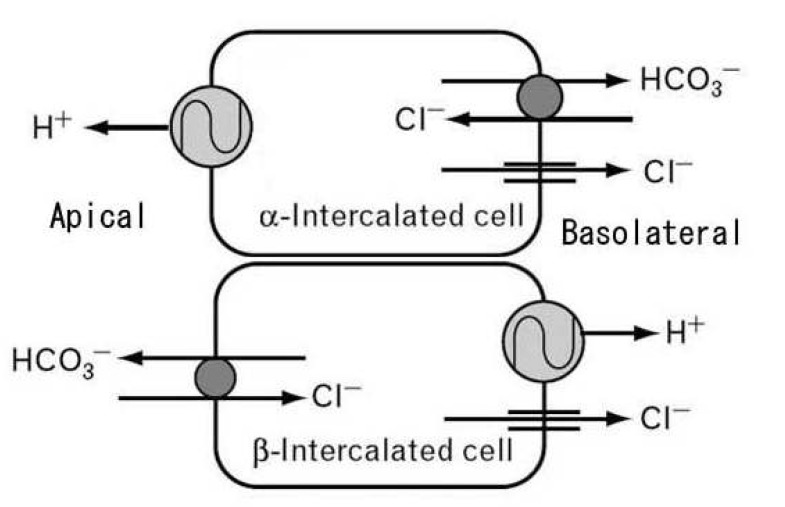
Fig. 1 Intercalated cells of collecting ducts. Collecting ducts have 2 types of intercalated cells: acid or hydrogen ion-secreting alpha-intercalated cell and bicarbonate-secreting beta-intercalated cell.
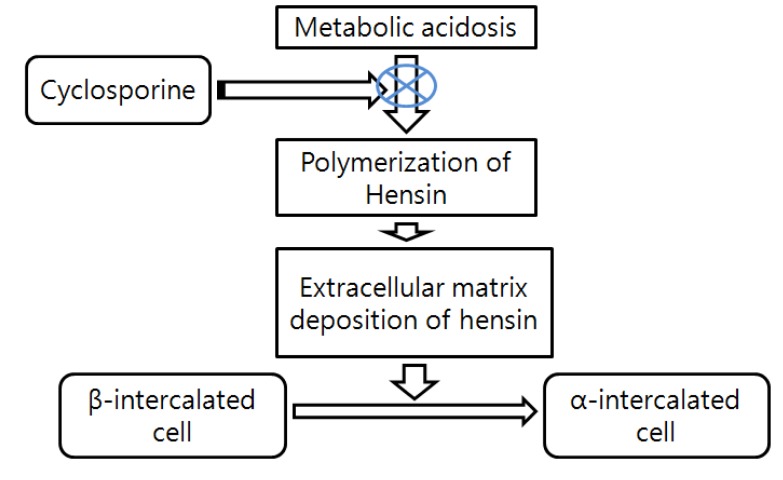
Fig. 2 Presumed mechanism of cyclosporine-induced metabolic acidosis. Cyclosporine inhibits polymerization of hensin protein, consequently acid-secreting cells will be less and then become at risk for mild normal anion gap metabolic acidosis.
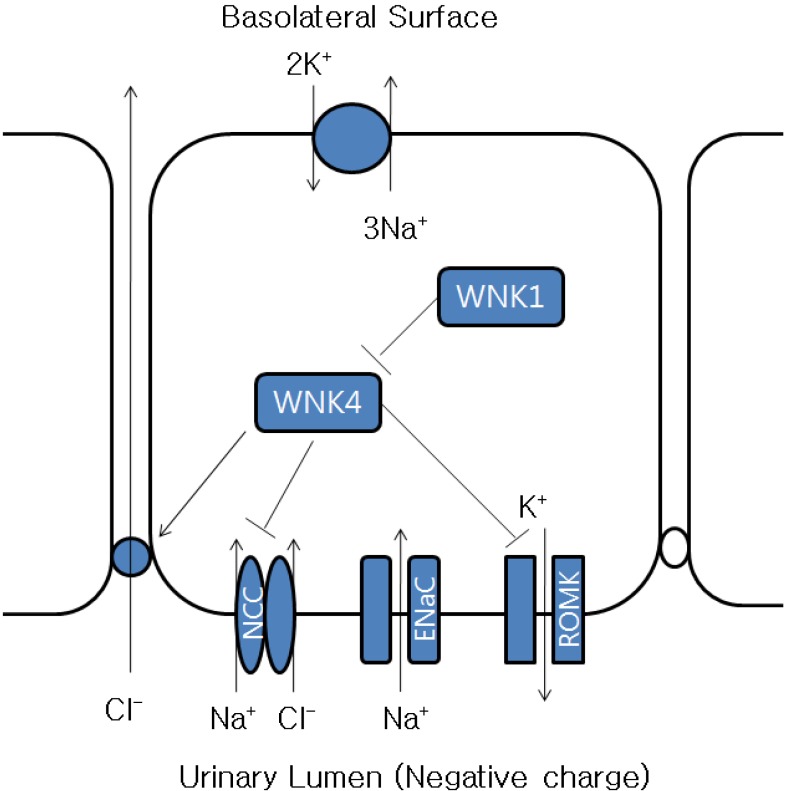
Fig. 3 Chloride shunt theory and clacineurin inhibitors. Calcineurin inhibitors inhibit the luminal potassium channel and increase chloride reabsorption.
Reference
-
1. Burdmann EA, Andoh TF, Yu L, Bennett WM. Cyclosporine nephrotoxicity. Semin Nephrol. 2003; 23:465–476. PMID: 13680536.
Article2. Massry SG, Preuss HG, Maher JF, Schreiner GE. Renal tubular acidosis after cadaver kidney homotransplantation. Studies on mechanism. Am J Med. 1967; 42:284–292. PMID: 5335111.3. Keven K, Ozturk R, Sengul S, Kutlay S, Ergun I, Erturk S, Erbay B. Renal tubular acidosis after kidney transplantation-incidence, risk factors and clinical implications. Nephrol Dial Transplant. 2007; 22:906–910. PMID: 17210594.
Article4. Yakupoglu HY, Corsenca A, Wahl P, Wüthrich RP, Ambühl PM. Posttransplant acidosis and associated disorders of mineral metabolism in patients with a renal graft. Transplantation. 2007; 84:1151–1157. PMID: 17998871.
Article5. Bartosh SM, Alonso EM, Whitington PF. Renal outcomes in pediatric liver transplantation. Clin Transplant. 1997; 11:354–360. PMID: 9361923.6. Schwarz C, Benesch T, Kodras K, Oberbauer R, Haas M. Complete renal tubular acidosis late after kidney transplantation. Nephrol Dial Transplant. 2006; 21:2615–2620. PMID: 16644772.
Article8. Schwartz GJ, Al-Awqati Q. Role of hensin in mediating the adaptation of the cortical collecting duct to metabolic acidosis. Curr Opin Nephrol Hypertens. 2005; 14:383–388. PMID: 15931009.
Article9. Watanabe S, Tsuruoka S, Vijayakumar S, Fischer G, Zhang Y, Fujimura A, Al-Awqati Q, Schwartz GJ. Cyclosporin A produces distal renal tubular acidosis by blocking peptidyl prolyl cis-trans isomerase activity of cyclophilin. Am J Physiol Renal Physiol. 2005; 288:F40–F47. PMID: 15353404.
Article10. Heering PJ, Kurschat C, Vo DT, Klein-Vehne N, Fehsel K, Ivens K. Aldosterone resistance in kidney transplantation is in part induced by a down-regulation of mineralocorticoid receptor expression. Clin Transplant. 2004; 18:186–192. PMID: 15016134.11. Bobadilla NA, Gamba G. New insights into the pathophysiology of cyclosporine nephrotoxicity: a role of aldosterone. Am J Physiol Renal Physiol. 2007; 293:F2–F9. PMID: 17429034.
Article12. Tsuruoka S, Schwartz GJ, Ioka T, Yamamoto H, Ando H, Fujimura A. Citrate reverses cyclosporin A-induced metabolic acidosis and bone resorption in rats. Am J Nephrol. 2005; 25:233–239. PMID: 15914972.
Article13. Kaplan B, Wang Z, Abecassis MM, Fryer JP, Stuart FP, Kaufman DB. Frequency of hyperkalemia in recipients of simultaneous pancreas and kidney transplants with bladder drainage. Transplantation. 1996; 62:1174–1175. PMID: 8900321.
Article14. Kim HC, Hwang EA, Han SY, Park SB, Kim HT, Cho WH. Primary immunosuppression with tacrolimus in kidney transplantation: three-year follow-up in a single center. Transplant Proc. 2004; 36:2082–2083. PMID: 15518753.
Article15. Deray G, Benhmida M, Le Hoang P, Maksud P, Aupetit B, Baumelou A, Jacobs C. Renal function and blood pressure in patients receiving long-term, low-dose cyclosporine therapy for idiopathic autoimmune uveitis. Ann Intern Med. 1992; 117:578–583. PMID: 1524331.
Article16. Kamel KS, Ethier JH, Quaggin S, Levin A, Albert S, Carlisle EJ, Halperin ML. Studies to determine the basis for hyperkalemia in recipients of a renal transplant who are treated with cyclosporine. J Am Soc Nephrol. 1992; 2:1279–1284. PMID: 1627752.
Article17. Tumlin JA, Sands JM. Nephron segment-specific inhibition of Na+/K(+)-ATPase activity by cyclosporin A. Kidney Int. 1993; 43:246–251. PMID: 8381891.
Article18. Aker S, Heering P, Kinne-Saffran E, Deppe C, Grabensee B, Kinne RK. Different effects of cyclosporine a and FK506 on potassium transport systems in MDCK cells. Exp Nephrol. 2001; 9:332–340. PMID: 11549851.
Article19. Deppe CE, Heering PJ, Tinel H, Kinne-Saffran E, Grabensee B, Kinne RK. Effect of cyclosporine A on Na+/K(+)-ATPase, Na+/K+/2Cl- cotransporter, and H+/K(+)-ATPase in MDCK cells and two subtypes, C7 and C11. Exp Nephrol. 1997; 5:471–480. PMID: 9438176.20. Ling BN, Eaton DC. Cyclosporin A inhibits apical secretory K+ channels in rabbit cortical collecting tubule principal cells. Kidney Int. 1993; 44:974–984. PMID: 8264157.21. Garzón-Muvdi T, Pacheco-Alvarez D, Gagnon KB, Vázquez N, Ponce-Coria J, Moreno E, Delpire E, Gamba G. WNK4 kinase is a negative regulator of K+-Cl- cotransporters. Am J Physiol Renal Physiol. 2007; 292:F1197–F1207. PMID: 17182532.22. Pei Y, Richardson R, Greenwood C, Wong PY, Baines A. Extrarenal effect of cyclosporine A on potassium homeostasis in renal transplant recipients. Am J Kidney Dis. 1993; 22:314–319. PMID: 8352259.
Article23. Gerstman BB, Kirkman R, Platt R. Intestinal necrosis associated with postoperative orally administered sodium polystyrene sulfonate in sorbitol. Am J Kidney Dis. 1992; 20:159–161. PMID: 1496969.
Article24. Moz Y, Levi R, Lavi-Moshayoff V, Cox KB, Molkentin JD, Silver J, Naveh-Many T. Calcineurin Abeta is central to the expression of the renal type II Na/Pi co-transporter gene and to the regulation of renal phosphate transport. J Am Soc Nephrol. 2004; 15:2972–2980. PMID: 15579499.25. Al-Khursany I, Thomas TH, Harrison K, Wilkinson R. Reduced erythrocyte and leukocyte magnesium is associated with cyclosporin treatment and hypertension in renal transplant patients. Nephrol Dial Transplant. 1992; 7:251–255. PMID: 1314999.
Article26. Barton CH, Vaziri ND, Martin DC, Choi S, Alikhani S. Hypomagnesemia and renal magnesium wasting in renal transplant recipients receiving cyclosporine. Am J Med. 1987; 83:693–699. PMID: 3314493.
Article27. Nijenhuis T, Hoenderop JG, Bindels RJ. Downregulation of Ca2+ and Mg2+ transport proteins in the kidney explains tacrolimus (FK506)-induced hypercalciuria and hypomagnesemia. J Am Soc Nephrol. 2004; 15:549–557. PMID: 14978156.28. Miura K, Nakatani T, Asai T, Yamanaka S, Tamada S, Tashiro K, Kim S, Okamura M, Iwao H. Role of hypomagnesemia in chronic cyclosporine nephropathy. Transplantation. 2002; 73:340–347. PMID: 11884928.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Antimicrobial-induced Electrolyte and Acid-Base Disturbances
- Electrolyte and Acid-Base Disturbances Associated with Non-Steroidal Anti-Inflammatory Drugs
- Study about Hypothermic - anesthesia during Intraperitoneal Hyperthermo - chemotherapeutic Perfusion Combined with Surgery in Far - advanced Stomach Cancer
- A comparison of traditional and quantitative analysis of acid-base and electrolyte imbalance in 87 cats
- Physiology and Pathophysiology of Transcellular Shift of Potassium Balance
