Acute Duodenal Ischemia and Periampullary Intramural Hematoma after an Uneventful Endoscopic Retrograde Cholangiopancreatography in a Patient with Primary Myelofibrosis
- Affiliations
-
- 1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea. sean4h@korea.ac.kr
- KMID: 2049026
- DOI: http://doi.org/10.5946/ce.2014.47.3.270
Abstract
- Acute duodenal ischemia and periampullary intramural hematoma are rare complications after endoscopic retrograde cholangiopancreatography (ERCP). A 77-year-old man with splenomegaly complained of abdominal pain caused by common bile duct (CBD) stone. After successful removal of the CBD stone without immediate complications, the patient developed intramural hematoma around the ampulla of Vater along with diffuse duodenal edema. The findings were compatible with acute intestinal ischemia, and further evaluation revealed that he had underlying primary myelofibrosis. Myeloproliferative diseases are known to be significantly associated with an increased risk of thrombohemorrhagic complications. Therefore, particular attention should be given to this group of patients when a high-risk procedure such as ERCP is performed.
Keyword
MeSH Terms
Figure
-
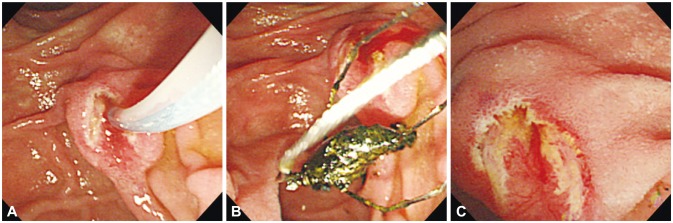
Fig. 1 (A) No bleeding occurred after endoscopic sphincterotomy. (B) A black pigment stone is successfully removed using a basket and (C) immediate complications are not observed after the procedure.
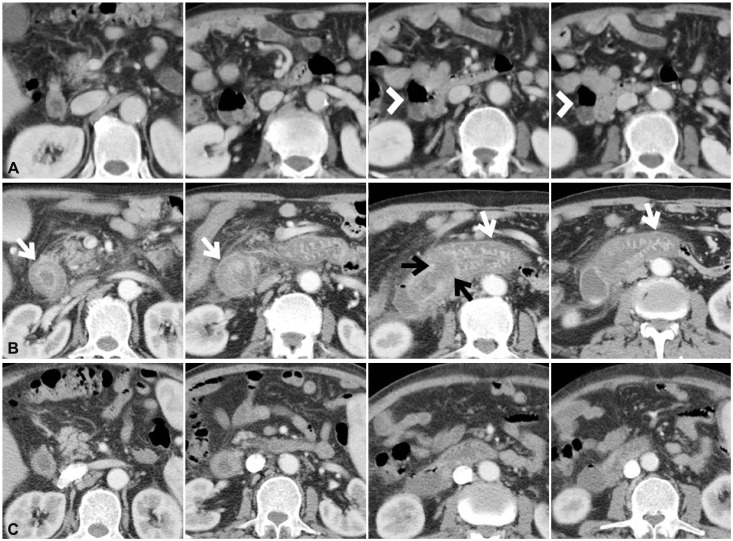
Fig. 2 (A) Initial abdomen computed tomography (CT) reveals a large duodenal diverticulum (arrowheads) on the lateral wall of duodenum second portion. (B) Abdominal CT performed the next day after endoscopic retrograde pancreaticoduodenography (ERCP) shows severe edematous wall thickening of the duodenum (white arrows). Localized focal low-attenuated lesion suggesting hematoma is also observed at the periampullary area (black arrows). (C) Follow-up abdominal CT performed 11 days after ERCP demonstrates considerably improved edematous wall thickening of the duodenum and resolved focal low-attenuated lesion at the periampullary area.
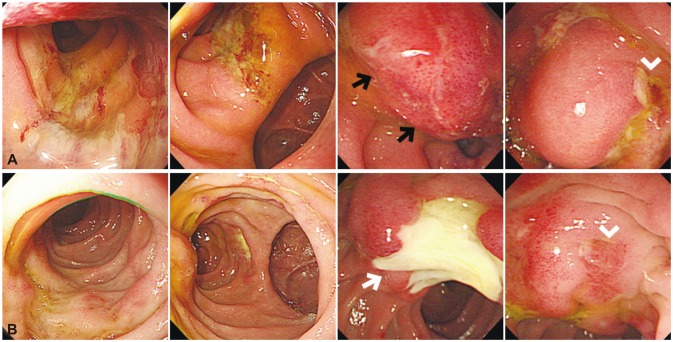
Fig. 3 (A) Endoscopic examination performed the day after endoscopic retrograde cholangiopancreatography (ERCP) demonstrates diffusely edematous duodenal mucosa with linear ulcerations and a large bulging lesion suggestive of hematoma (black arrows) distal to the ampulla of Vater (arrowhead). (B) Follow-up endoscopy performed 8 days after ERCP shows much improved duodenal wall edema with a large ulcer where the hematoma had been (white arrow).
Reference
-
1. Pannu HK, Fishman EK. Complications of endoscopic retrograde cholangiopancreatography: spectrum of abnormalities demonstrated with CT. Radiographics. 2001; 21:1441–1453. PMID: 11706215.
Article2. Barbui T, Finazzi G, Falanga A. Myeloproliferative neoplasms and thrombosis. Blood. 2013; 122:2176–2184. PMID: 23823316.
Article3. Melato M, Falconieri G, Manconi R, Bucconi S. Intramural gastric hematoma and hemoperitoneum occurring in a patient affected by idiopathic myelofibrosis. Hum Pathol. 1980; 11:301–302. PMID: 7399522.
Article4. Tefferi A. Primary myelofibrosis: 2013 update on diagnosis, risk-stratification, and management. Am J Hematol. 2013; 88:141–150. PMID: 23349007.
Article5. Tefferi A. Myelofibrosis with myeloid metaplasia. N Engl J Med. 2000; 342:1255–1265. PMID: 10781623.
Article6. Reilly JT, McMullin MF, Beer PA, et al. Guideline for the diagnosis and management of myelofibrosis. Br J Haematol. 2012; 158:453–471. PMID: 22651893.
Article7. Barbui T, Carobbio A, Cervantes F, et al. Thrombosis in primary myelofibrosis: incidence and risk factors. Blood. 2010; 115:778–782. PMID: 19965680.
Article8. Vannucchi AM. Management of myelofibrosis. Hematology Am Soc Hematol Educ Program. 2011; 2011:222–230. PMID: 22160038.9. Papadakis E, Hoffman R, Brenner B. Thrombohemorrhagic complications of myeloproliferative disorders. Blood Rev. 2010; 24:227–232. PMID: 20817333.
Article10. Leoni P, Rupoli S, Lai G, et al. Platelet abnormalities in idiopathic myelofibrosis: functional, biochemical and immunomorphological correlations. Haematologica. 1994; 79:29–39. PMID: 15378946.11. Finazzi G, Carobbio A, Thiele J, et al. Incidence and risk factors for bleeding in 1104 patients with essential thrombocythemia or prefibrotic myelofibrosis diagnosed according to the 2008 WHO criteria. Leukemia. 2012; 26:716–719. PMID: 21926959.
Article12. Diniz-Santos DR, de Andrade Cairo RC, Braga H, Araújo-Neto C, Paes IB, Silva LR. Duodenal hematoma following endoscopic duodenal biopsy: a case report and review of the existing literature. Can J Gastroenterol. 2006; 20:39–42. PMID: 16432559.13. Guzman C, Bousvaros A, Buonomo C, Nurko S. Intraduodenal hematoma complicating intestinal biopsy: case reports and review of the literature. Am J Gastroenterol. 1998; 93:2547–2550. PMID: 9860424.
Article14. ASGE Standards of Practice Committee. Anderson MA, Ben-Menachem T, et al. Management of antithrombotic agents for endoscopic procedures. Gastrointest Endosc. 2009; 70:1060–1070. PMID: 19889407.
Article15. Bobadilla JL. Mesenteric ischemia. Surg Clin North Am. 2013; 93:925–940. PMID: 23885938.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intramural Duodenal Hematoma after Transpancreatic Septotomy during ERCP: A Case Report and Literature Review
- The Management of Endoscopic Retrograde Cholangiopancreatography-Related Duodenal Perforation
- Four Cases of Guidewire Induced Periampullary Perforation During Endoscopic Retrograde Cholangiopancreatography
- Successful Endoscopic Decompression for Intramural Duodenal Hematoma with Gastric Outlet Obstruction Complicating Acute Pancreatitis
- A Case of Intramural Duodenal Hematoma after the Use of the Endoscopic Epinephrine Injection Method for Duodenal Ulcer Bleeding in a Chronic Renal Failure Patient undergoing Maintenance Hemodialysis
