Submucosal Endoscopy, a New Era of Pure Natural Orifice Translumenal Endoscopic Surgery (NOTES)
- Affiliations
-
- 1Department of Internal Medicine, Soonchunhyang University Cheonan Hospital, Soonchunhyang University College of Medicine, Cheonan, Korea.
- 2NOTES Study Group in Korean Society of Gastrointestinal Endoscopy, Seoul, Korea. cjy6695@dreamwiz.com
- 3Department of Internal Medicine, Soonchunhyang University Seoul Hospital, Soonchunhyang University College of Medicine, Seoul, Korea.
- KMID: 2048829
- DOI: http://doi.org/10.5946/ce.2012.45.1.4
Abstract
- Natural orifice translumenal endoscopic surgery (NOTES) involves the intentional perforation of the viscera with an endoscope to access the abdominal cavity and perform an intraabdominal operation. In a brief time period, NOTES has been shown to be feasible in laboratory animal and human studies. Easy access to the peritoneal cavity and complete gastric closure should be secured before NOTES can be recommended as an acceptable alternative in clinical practice. The concept of submucosal endoscopy has been introduced as a solution to overcome these two primary barriers to human NOTES application. Its offset entry/exit access method effectively prevents contamination and allows the rapid closure of the entry site with a simple mucosal apposition. In addition, it could be used as an endoscopic working space for various submucosal conditions. Herein, the detailed procedures, laboratory results and human application of the submucosal endoscopy will be reviewed.
Keyword
Figure
-

Fig. 1 Schematic drawings of submucosal endoscopy with mucosal flap technique. (A) The submucosal plane is isolated with injection of CO2 gas injection, (B) repeated balloon dissection of the submucosa. (C) The endoscope is inserted into the submucosal space, a myotomy exit site is made with modified cap EMR technique. (D) The peritoneal cavity is accessed via the myotomy. (E) The endoscopic entry point into the submucosal space is closed (Adopted from Sumiyama et al. Minim Invasive Ther Allied Technol 2008;17:365-369).3
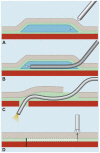
Fig. 2 Schematic drawings of modified endoscopic submucosal dissection (ESD) technique. (A) Submucosal injection with normal saline solution. (B) Creation of a longitudinal narrow submucosal tunnel using ESD. (C) Advancement of an endoscope into the peritoneal cavity. (D) Closure of the mucosal incision site using endoclips (Adopted from Yoshizumi et al. Endoscopy 2009;41:707-711).4
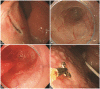
Fig. 3 Peroral transgastric peritoneoscopy. (A) A mucosal incision at the submucosal bleb. (B) A submucosal tunnel created using endoscopic submucosal dissection. (C) Balloon dilation after a small puncture of the seromuscular layer. (D) Endoscopic forceps biopsy from the metastatic nodules in the peritoneum.
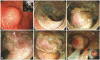
Fig. 4 Endoscopic full-thickness resection of subepitherial tumor (SET). (A) A SET at the anterior wall of the low body. (B) A submucosal tunnel created using endoscopic submucosal dissection. (C) The exposed tumor within the submucosal tunnel. (D) Full-thickness incision around the tumor. (E) Full-thickness dissection of the seromuscular layer. (F) The final snare resection of the tumor.

Fig. 5 Peroral endoscopic myotomy. (A) Entry to submucosal space. (B) Submucosal tunneling. (C) Endoscopic myotomy, with a total length of 10 cm. (D) Long endoscopic myotomy of inner circular muscle bundles, leaving the outer longitudinal muscle layer intact. (E) Closure of mucosal entry (Adopted from Inoue et al. Endoscopy 2010;42:265-271).16
Cited by 2 articles
-
International Digestive Endoscopy Network 2012: A Patchwork of Networks for the Future
Kwang An Kwon, Il Ju Choi, Eun Young Kim, Seok Ho Dong, Ki Baik Hahm
Clin Endosc. 2012;45(3):209-210. doi: 10.5946/ce.2012.45.3.209.Preparation and Patient Evaluation for Safe Gastrointestinal Endoscopy
Seong Hee Kang, Jong Jin Hyun
Clin Endosc. 2013;46(3):212-218. doi: 10.5946/ce.2013.46.3.212.
Reference
-
1. Kalloo AN, Singh VK, Jagannath SB, et al. Flexible transgastric peritoneoscopy: a novel approach to diagnostic and therapeutic interventions in the peritoneal cavity. Gastrointest Endosc. 2004; 60:114–117. PMID: 15229442.
Article2. Sumiyama K, Gostout CJ, Rajan E, Bakken TA, Knipschield MA. Transesophageal mediastinoscopy by submucosal endoscopy with mucosal flap safety valve technique. Gastrointest Endosc. 2007; 65:679–683. PMID: 17383463.
Article3. Sumiyama K, Tajiri H, Gostout CJ. Submucosal endoscopy with mucosal flap safety valve (SEMF) technique: a safe access method into the peritoneal cavity and mediastinum. Minim Invasive Ther Allied Technol. 2008; 17:365–369. PMID: 18972253.
Article4. Yoshizumi F, Yasuda K, Kawaguchi K, Suzuki K, Shiraishi N, Kitano S. Submucosal tunneling using endoscopic submucosal dissection for peritoneal access and closure in natural orifice transluminal endoscopic surgery: a porcine survival study. Endoscopy. 2009; 41:707–711. PMID: 19670139.
Article5. Gee DW, Willingham FF, Lauwers GY, Brugge WR, Rattner DW. Natural orifice transesophageal mediastinoscopy and thoracoscopy: a survival series in swine. Surg Endosc. 2008; 22:2117–2122. PMID: 18636291.
Article6. Sumiyama K, Gostout CJ, Rajan E, et al. Pilot study of transesophageal endoscopic epicardial coagulation by submucosal endoscopy with the mucosal flap safety valve technique (with videos). Gastrointest Endosc. 2008; 67:497–501. PMID: 18294512.
Article7. Pauli EM, Mathew A, Haluck RS, et al. Technique for transesophageal endoscopic cardiomyotomy (Heller myotomy): video presentation at the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) 2008, Philadelphia, PA. Surg Endosc. 2008; 22:2279–2280. PMID: 18622556.
Article8. Pasricha PJ, Hawari R, Ahmed I, et al. Submucosal endoscopic esophageal myotomy: a novel experimental approach for the treatment of achalasia. Endoscopy. 2007; 39:761–764. PMID: 17703382.
Article9. Pauli EM, Moyer MT, Haluck RS, Mathew A. Self-approximating transluminal access technique for natural orifice transluminal endoscopic surgery: a porcine survival study (with video). Gastrointest Endosc. 2008; 67:690–697. PMID: 18279870.
Article10. Sumiyama K, Gostout CJ, Rajan E, et al. Transgastric cholecystectomy: transgastric accessibility to the gallbladder improved with the SEMF method and a novel multibending therapeutic endoscope. Gastrointest Endosc. 2007; 65:1028–1034. PMID: 17531637.
Article11. von Delius S, Gillen S, Doundoulakis E, et al. Comparison of transgastric access techniques for natural orifice transluminal endoscopic surgery. Gastrointest Endosc. 2008; 68:940–947. PMID: 18561921.
Article12. Moyer MT, Pauli EM, Gopal J, Mathew A, Haluck RS. Durability of the self-approximating translumenal access technique (STAT) for potential use in natural orifice translumenal surgery (NOTES). Surg Endosc. 2011; 25:315–321. PMID: 20725749.
Article13. Lee CK, Lee SH, Chung IK, et al. Human diagnostic transgastric peritoneoscopy with the submucosal tunnel technique performed with the patient under conscious sedation (with video). Gastrointest Endosc. 2010; 72:889–891. PMID: 20510412.
Article14. Kitano S, Yasuda K, Shibata K, et al. Natural orifice translumenal endoscopic surgery for preoperative staging in a pancreatic cancer patient. Dig Endosc. 2008; 20:198–202.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Natural Orifice Translumenal Endoscopic Surgery (NOTES) Applied Totally to Sigmoidectomy: An Original Technique with Survival in a Porcine Model (Surgical Endoscopy 2009;23:24-30)
- Natural Orifice Transluminal Endoscopic Surgery and Upper Gastrointestinal Tract
- Natural Orifice Transluminal Endoscopic Surgery in Korea
- Natural Orifice Transluminal Endoscopic Surgery (NOTES): Current Status and Future Prospects
- Natural Orifice Transluminal Endoscopic Surgery (NOTES)
