Anat Cell Biol.
2013 Dec;46(4):296-298. 10.5115/acb.2013.46.4.296.
Sessile ileum, subhepatic cecum, and uncinate appendix that might lead to a diagnostic dilemma
- Affiliations
-
- 1Department of Anatomy, Melaka Manipal Medical College (Manipal Campus), Manipal University, Manipal, Karnataka, India. nayaksathish@gmail.com
- KMID: 2046771
- DOI: http://doi.org/10.5115/acb.2013.46.4.296
Abstract
- The subhepatic position of the cecum and appendix is a result of embryological reasons. Subhepatic appendicitis can cause diagnostic dilemmas. During the dissection of an adult male cadaver aged approximately 70 years, the subhepatic position of the cecum and appendix was noted. The appendix made a "U"-shaped bend and its tip was located in the paracolic position. The cecum had appendices epiploicae, and the terminal part of the ileum was retroperitoneal and had ascended vertically to the cecum from the right iliac fossa. Functionally, the sessile part of the ileum might restrict its peristaltic movements. The abnormal position of the terminal ileum might be mistaken for an ascending colon during laparoscopic surgery. The subhepatic position of the cecum and appendix might cause confusion in the diagnosis of acute appendicitis because the tenderness in such cases is not located at the McBurney's point.
Keyword
MeSH Terms
Figure
-
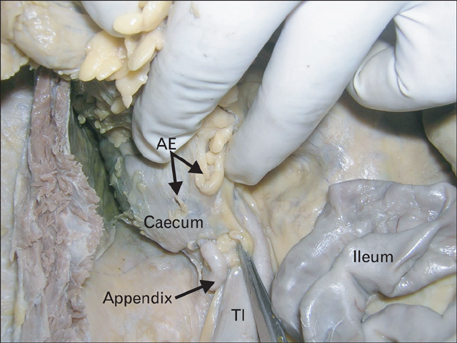
Fig. 1 Closer view of the cecum and appendix. Note the vertical course of the terminal ileum (TI) before opening into the cecum. Appendices epiploicae (AE) are also seen.

Fig. 2 The cecum and appendix have been mobilized to show their relationship to the right kidney (RK) and right lobe of the liver (RLL). Note the terminal part of the ileum (TI) joining the cecum vertically.
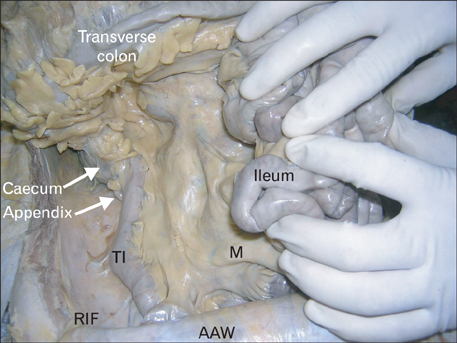
Fig. 3 Photograph of the subhepatic position of cecum and appendix. The anterior abdominal wall (AAW) has been reflected, and the ileum has been pulled to the left. Note the right iliac fossa (RIF), the sessile terminal part of ileum (TI), and the mesentery (M) of the small intestine.
Reference
-
1. Snell RS. Clinical anatomy. 7th ed. Baltimore: Lippincott Williams & Wilkins;2004. p. 215–217.2. BEACH Program. AIHW General Practice Statistics and Classification Unit. Presentations of abdominal pain in Australian general practice. Aust Fam Physician. 2004; 33:968–969.3. Schumpelick V, Dreuw B, Ophoff K, Prescher A. Appendix and cecum: embryology, anatomy, and surgical applications. Surg Clin North Am. 2000; 80:295–318.4. Kulvatunyou N, Schein M. Perforated subhepatic appendicitis in the laparoscopic era. Surg Endosc. 2001; 15:769.5. King A. Subhepatic appendicitis. AMA Arch Surg. 1955; 71:265–267.6. Standring S. Gray's anatomy: the anatomical basis of clinical practice. 39th ed. New York: Elsevier Churchill Livingstone;2005.7. Ahmadpour SH, Nasirizadeh S, Gorjifard M. Abnormal retroperitoneal ileum, undscended ileucecal junction and subhepatic appendix in a macrosomatic fetus: a case report. J Morphol Sci. 2012; 29:120–122.8. Applegate KE, Anderson JM, Klatte EC. Intestinal malrotation in children: a problem-solving approach to the upper gastrointestinal series. Radiographics. 2006; 26:1485–1500.9. Awapittaya B, Pattana-arun J, Tansatit T, Kanjanasilpa P, Sahakijrungruang C, Rojanasakul A. New concept of ileocecal junction: intussusception of the terminal ileum into the cecum. World J Gastroenterol. 2007; 13:2855–2857.10. Patel NR, Lakshman S, Hays TV, Thomas E. Subhepatic appendix with fecalith mimicking acute cholecystitis with gallstone. J Clin Ultrasound. 1996; 24:45–47.
