Imaging Findings of Endometrial Metastasis from Colon Cancer: A Case Report
- Affiliations
-
- 1Department of Radiology, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea. pksungbin@paran.com
- 2Department of Pathology, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea.
- 3Department of Internal Medicine, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea.
- 4Department of Nuclear Medicine, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea.
- KMID: 2041951
- DOI: http://doi.org/10.3348/jksr.2013.69.4.301
Abstract
- Metastasis to the uterus is thought to be a very rare condition, and few imaging findings have been reported in the English literature. Here, we describe a case of endometrial metastasis from colon cancer, which was depicted using gray-scale and Doppler ultrasonography, CT and positron emission tomography-CT, to be a smoothly lobulated heterogeneous, predominantly endometrial mass in the uterus with increased vascular flow.
MeSH Terms
Figure
-
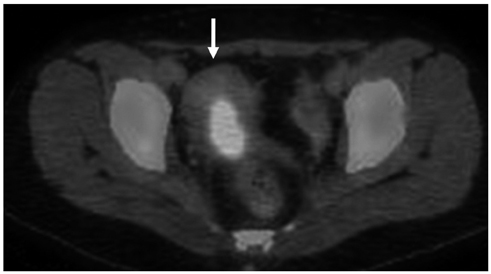
Fig. 1 Axial image of PET-CT shows a hypermetabolic lesion in the uterus (arrow, max-SUV: 13.2). The uterine lesion was thought to be due to a menstrual physiologic uptake, rather than true lesion. Note.-max-SUV = maximal standardized uptake value, PET-CT = positron emission tomography-CT

Fig. 2 Axial image of contrast-enhanced abdomen and pelvis CT scan shows heterogeneously enhancing lesion in the uterus (arrow). Lymph node enlargement is also noted in left external iliac area (not shown).
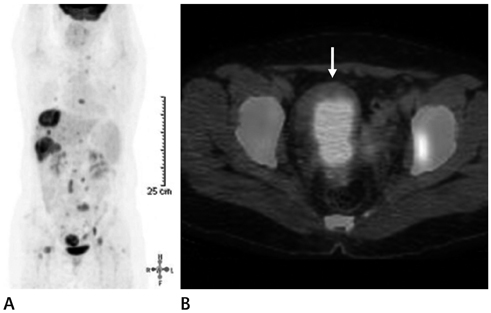
Fig. 3 Follow-up PET-CT scan after eight months. A. After eight months follow-up, whole-body PET-CT scan shows multiple hepatic metastases with newly developed hypermetabolic metastatic lesions in both lungs, multiple bones, lymph nodes (paraaortic and left pelvic lymph nodes), and peritoneum. B. Follow-up axial image of PET-CT shows the increased size of the hypermetabolic lesion in the uterus (arrow, max-SUV: 10.9), compared with previous PET-CT (Fig. 1). Note.-max-SUV = maximal standardized uptake value, PET-CT = positron emission tomography-CT

Fig. 4 Gray-scale and Doppler endovaginal US images. A. Gray-scale endovaginal US demonstrates a 4.0 × 1.4 cm, smoothly lobulated heterogeneous mass located predominantly in the uterine endometrium with endocervical extension (arrow). B. Doppler endovaginal US shows increased vascular flow within the mass (arrow). Note.-US = ultrasonography
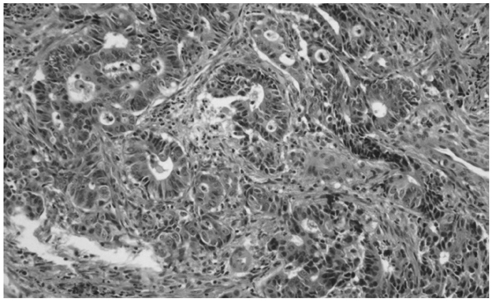
Fig. 5 Photomicrograph of a histologic specimen from endometrial curettage showing gland-forming atypical cell infiltration with neoplastic glands adjacent to normal endometrial glands (hematoxylin-eosin, × 200). The histopathology findings were consistent with metastasis from colonic adenocarcinoma as identified from the previous hemicolectomy specimen. The immunohistochemical profile revealed positive staining for CK20 and negative for CK, which was strongly suggestive of colonic adenocarcinoma (not shown).
Reference
-
1. Mazur MT, Hsueh S, Gersell DJ. Metastases to the female genital tract. Analysis of 325 cases. Cancer. 1984; 53:1978–1984.2. Metser U, Haider MA, Khalili K, Boerner S. MR imaging findings and patterns of spread in secondary tumor involvement of the uterine body and cervix. AJR Am J Roentgenol. 2003; 180:765–769.3. Kumar NB, Hart WR. Metastases to the uterine corpus from extragenital cancers. A clinicopathologic study of 63 cases. Cancer. 1982; 50:2163–2169.4. Lemoine NR, Hall PA. Epithelial tumors metastatic to the uterine cervix. A study of 33 cases and review of the literature. Cancer. 1986; 57:2002–2005.5. Weingold AB, Boltuch SM. Extragenital metastases to the uterus. Am J Obstet Gynecol. 1961; 82:1267–1272.6. Daw E. Extragenital adenocarcinoma metastatic to the cervix uteri. Am J Obstet Gynecol. 1972; 114:1104–1105.7. Tarraza HM, Muntz HG, De Cain M, Jones MA. Cervical metastases in advanced ovarian malignancies. Eur J Gynaecol Oncol. 1993; 14:274–278.8. Zannoni GF, Vellone VG, Fadda G, Petrillo M, Scambia G. Colonic carcinoma metastatic to the endometrium: the importance of clinical history in averting misdiagnosis as a primary endometrial carcinoma. Int J Surg Pathol. 2011; 19:787–790.9. Derchi LE, Serafini G, Gandolfo N, Gandolfo NG, Martinoli C. Ultrasound in gynecology. Eur Radiol. 2001; 11:2137–2155.10. Blake MA, Singh A, Setty BN, Slattery J, Kalra M, Maher MM, et al. Pearls and pitfalls in interpretation of abdominal and pelvic PET-CT. Radiographics. 2006; 26:1335–1353.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diagnosis of Cardiac Metastasis from Endometrial Cancer by F-18 FDG-PET/CT
- Isolated Small Bowel Metastasis of Endometrial Carcinoma with Resultant Jejunojejunal Intussusception: A Case Report
- Endoscopic therapy of early colon cancer
- A Case of Endometrial Cancer with Hereditary Non-Polyposis Colorectal Cancer (HNPCC)
- A Case of Complete Response by Hormonal Therapy with Tamoxifen and Progesterone in Recurrent Endometrial Cancer to Metastasis to Lung
