Petrous Apex Cephalocele: Report of Two Cases and Review of the Literature
- Affiliations
-
- 1Department of Diagnostic Radiology, Seoul Paik Hospital, Inje University College of Medicine, Seoul, Korea. hongage@unitel.co.kr
- KMID: 2040811
- DOI: http://doi.org/10.3348/jksr.2011.64.5.439
Abstract
- A petrous apex cephalocele is a rare lesion of the petrous apex. It can be discovered incidentally or can cause a suite of clinical problems, such as trigeminal neuralgia or cerebrospinal fluid leakage. Although this lesion can be misinterpreted as a pathologic lesion, the characteristic radiologic features can provide the diagnostic clue for distinguishing these two lesions and avoid unnecessary treatment. Here we present CT and MRI finding of petrous apex cephalocele in two patients with review of the literature.
MeSH Terms
Figure
-

Fig. 1 Axial temporal bone CT image (A) shows sharply marginated, multilobulating erosive lesions (arrows) at the bilateral petrous apex with a thin cortical bone outline (Right : 2.7 × 1.0 cm, Left : 1.6 × 1.0 cm). Axial T1-(B), T2-weighted (C), and FLAIR image (D) demonstrate CSF signal intensity at the bilateral petrous apex, contiguous to Meckel's cave (arrows in C). On contrast-enhanced T1-weighted images (E), thin wall enhancement is noted at the bilateral petrous apex lesions (curved arrows) and DWI (F) as well as ADC maps (G), which reveal the CSF-like content of lesions (arrows in F). A sagittal T1-weighted image (H) shows combined empty sella (arrow).
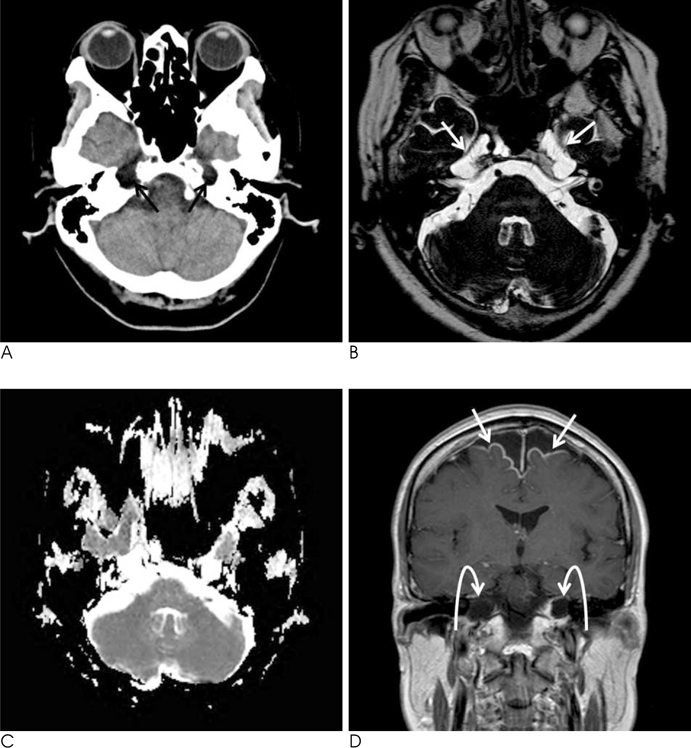
Fig. 2 Axial brain CT image (A) shows cystic lesions (black arrows) at the bilateral petrous apex. The DRIVE sequence (B) demonstrates bilateral petrous apex lesions more clearly, which are cystic and contiguous to Meckel's cave (arrows). ADC maps (C) also reveal the CSF-like content of the lesions. On a contrast-enhanced T1-weighted coronal image (D) shows localized meningeal enhancement at a high frontal area near the midline (arrows), but the lesions at the bilateral petrous apex (curved arrows) were not enhanced.
Reference
-
1. Muckle RP, De la Cruz A, Lo WM. Petrous apex lesions. Am J Otol. 1998; 19:219–225.2. Isaacson B, Kutz JW, Roland PS. Lesions of the petrous apex: diagnosis and management. Otolaryngol Clin North Am. 2007; 40:479–519.3. Alorainy IA. Petrous apex cephalocele and empty sella: is there any relation. Eur J Radiol. 2007; 62:378–384.4. Moore KR, Fischbein NJ, Harnsberger HR, Shelton C, Glastonbury CM, White DK, et al. Petrous apex cephalocele. AJNR Am J Neuroradiol. 2001; 22:1867–1871.5. Achilli V, Danesi G, Caverni L, Richichi M. Petrous apex arachnoid cyst: a case report and review of the literature. Acta Otorhinolaryngol Ital. 2005; 25:296–300.6. Isaacson B, Coker NJ, Vrabec JT, Yoshor D, Oghalai JS. Invasive cerebrospinal fluid cysts and cephaloceles of the petrous apex. Otol Neurotol. 2006; 27:1131–1141.7. Batra A, Tripathi RP, Singh AK, Tatke M. Petrous apex arachnoid cyst extending into Mecke's cave. Australas Radiol. 2002; 46:295–298.8. Motojima T, Fujii K, Ishiwada N, Takanashi J, Numata O, Uchino Y, et al. Recurrent meningitis associated with a petrous apex cephalocele. J Child Neurol. 2005; 20:168–170.9. Sage MR, Blumbergs PC. Primary empty sella turcica: a radiological-anatomical correlation. Australasian Radiology. 2000; 44:341–348.10. Moore KR, Harnsberger HR, Shelton C, Davidson HC. "Leave me alone" lesions of the petrous apex. AJNR Am J Neuroradiol. 1998; 19:733–738.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Anatomy for the Infracochlear Approach to the Petrous Apex
- A Case of Huge Congenital Cholesteatoma of Petrous Apex Treated With Translabyrinthine Marsupialization
- Petrous Apex Pneumatization on Computed Tomography
- Surgical Anatomical Landmarks for Petrous Apex
- New Technique for Surgery of Petrous Apex Cholesterol Granuloma
