Surgical treatment of atrial fibrillation
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. jwlee@amc.seoul.kr
- KMID: 2015676
- DOI: http://doi.org/10.5124/jkma.2013.56.9.805
Abstract
- Despite its proven efficacy in the treatment of atrial fibrillation (AF), the Cox-Maze III procedure has not been widely accepted owing to its complexity and technical difficulty. New ablation technologies have led to the development of various simplified lesion sets, including minimally invasive techniques. Given recent improvements in the percutaneous catheter ablation technique, it seems to have replaced surgical treatment of AF, especially for lone AF. However, suboptimal results of catheter ablation have been reported, and it has been well established that the Cox-Maze III procedure is still the gold standard for surgical AF ablation. Nevertheless, many physicians and patients are reluctant to undergo surgery for lone AF because of its invasiveness. In this regard, improvements in minimally invasive technology should be directed toward replicating the original Cox-Maze III technique and ultimately on performing it on the beating heart without cardiopulmonary bypass. This review provides an overview of the current state of the art and future directions in the surgical treatment of AF. Based on a better understanding of the mechanisms of AF and various treatment techniques, and improvements in diagnostic techniques, the appropriate option among various surgical techniques should be selected tailored to individual patients, making the surgical treatment of AF available to a larger population of patients.
Keyword
Figure
-

Figure 1 The traditional cut-and-sew Cox-Maze III procedure (From Cox JL, et al. J Thorac Cardiovasc Surg 1991;101:569-583, with permission from Elsevier) [13].
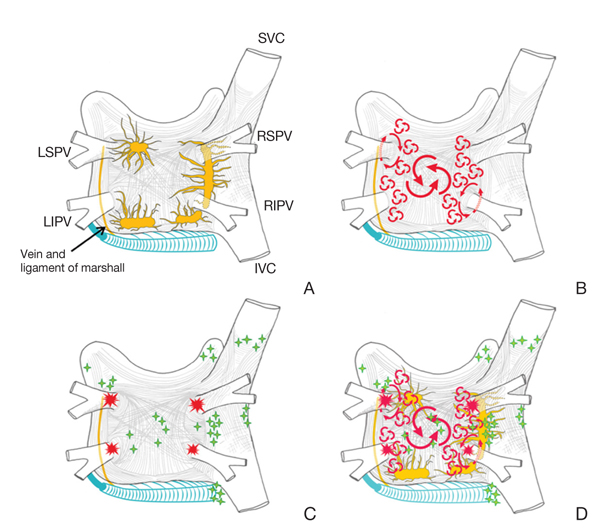
Figure 2 Structure and mechanisms of atrial fibrillation. (A) Schematic drawing of the left and right atria as viewed from the posterior. The extension of muscular fibers onto the pulmonary veins can be appreciated. Shown in yellow are the five major left atrial autonomic ganglionic plexi and axons. Shown in blue is the coronary sinus, which is enveloped by muscular fibers that have connections to the atria. Also shown in blue is the vein and ligament of Marshall, which travels from the coronary sinus to the region between the left superior pulmonary vein (LSPV) and the left atrial appendage. (B) The large and small reentrant wavelets that play a role in initiating and sustaining atrial fibrillation. (C) The common locations of pulmonary veins (red) and also the common sites of origin of non-pulmonary vein triggers (green). (D) Composite of the anatomic and arrhythmic mechanisms of atrial fibrillation. SVC, superior vena cava; RSPV, right superior pulmonary vein; LIPV, left inferior pulmonary vein; RIPV, right inferior pulmonary vein; IVC, inferior vena cava (From Calkins H, et al. Heart Rhythm 2012;9: 632.e21-696.e21, with permission from Elsevier) [10].
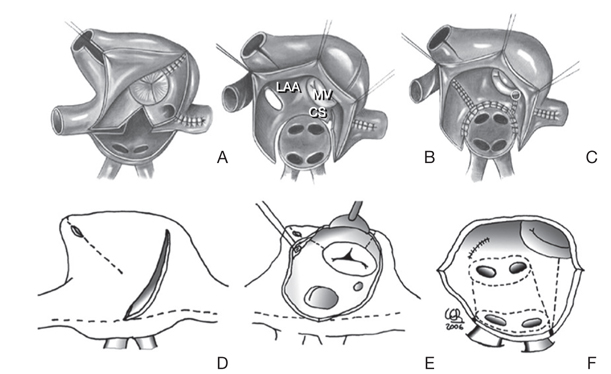
Figure 3 Similar line patterns, different type of lesions. (A), (B), and (C) show the lines described by Cox in the cut-and-sew Cox-Maze III. (D), (E), and (F) show pattern for a Cox-Maze IV, combining incisions and bipolar radifrequency ablation (dotted lines). LAA, left atrial appendage; MV, mitral valve; CS, coronary sinus (From Castella M, et al. J Thorac Cardiovasc Surg 2008;136:419-423, with permission from Elsevier) [14].

Figure 4 Diagram of the left atrial (A) and right atrial (B) ablation procedures using cryoablation (dotted lines). SVC, superior vena cava; LAA, left atrial appendage; PV, pulmonary vein; MV, mitral valve; IVC, inferior vena cava; RAA, right atrial appendage; TV, tricuspid valve; CS, coronary sinus (From Kim JB, et al. Ann Thorac Surg 2011;92:1397-1404, with permission from Elsevier) [22].

Figure 5 The Dallas epicardial lesion set for minimal access left atrial maze. 1, 2 and 3 indicates position of the temporary pacing and recording electrodes for intraoperative physiological evaluation to insure complete isolation across each lesion line. LAA, left atrial appendage; PV, pulmonary vein; LA, left atrial (From Edgerton JR, et al. Ann Thorac Surg 2009;88:1655-1657, with permission from Elsevier) [27].
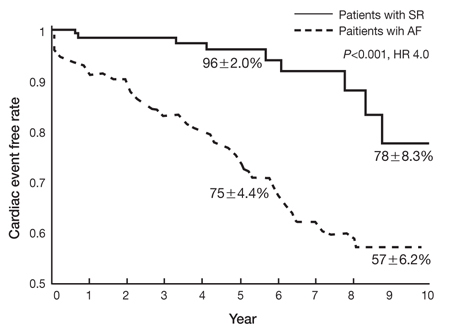
Figure 6 A significant difference in cardiac event-free rate was observed between patients with preoperative sinus rhythm and atrial fibrillation (AF) undergoing degenerative mitral valve repair. SR, sinus rhythm; HR, hazard ratio (From Eguchi K, et al. Eur Heart J 2005;26:1866-1872, with permission from Elsevier) [32].
Reference
-
1. Feinberg WM, Blackshear JL, Laupacis A, Kronmal R, Hart RG. Prevalence, age distribution, and gender of patients with atrial fibrillation. Analysis and implications. Arch Intern Med. 1995; 155:469–473.
Article2. Friberg J, Scharling H, Gadsboll N, Jensen GB. Sex-specific increase in the prevalence of atrial fibrillation (The Copenhagen City Heart Study). Am J Cardiol. 2003; 92:1419–1423.
Article3. Furberg CD, Psaty BM, Manolio TA, Gardin JM, Smith VE, Rautaharju PM. Prevalence of atrial fibrillation in elderly subjects (the Cardiovascular Health Study). Am J Cardiol. 1994; 74:236–241.
Article4. Hart RG, Halperin JL. Atrial fibrillation and thromboembolism: a decade of progress in stroke prevention. Ann Intern Med. 1999; 131:688–695.
Article5. Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation: a major contributor to stroke in the elderly. The Framingham Study. Arch Intern Med. 1987; 147:1561–1564.
Article6. Cox JL. Atrial fibrillation I: a new classification system. J Thorac Cardiovasc Surg. 2003; 126:1686–1692.
Article7. Cox JL, Jaquiss RD, Schuessler RB, Boineau JP. Modification of the maze procedure for atrial flutter and atrial fibrillation. II. Surgical technique of the maze III procedure. J Thorac Cardiovasc Surg. 1995; 110:485–495.
Article8. Prasad SM, Maniar HS, Camillo CJ, Schuessler RB, Boineau JP, Sundt TM 3rd, Cox JL, Damiano RJ Jr. The Cox maze III procedure for atrial fibrillation: long-term efficacy in patients undergoing lone versus concomitant procedures. J Thorac Cardiovasc Surg. 2003; 126:1822–1828.
Article9. Cox JL. The central controversy surrounding the interventional-surgical treatment of atrial fibrillation. J Thorac Cardiovasc Surg. 2005; 129:1–4.
Article10. Calkins H, Kuck KH, Cappato R, Brugada J, Camm AJ, Chen SA, Crijns HJ, Damiano RJ Jr, Davies DW, DiMarco J, Edgerton J, Ellenbogen K, Ezekowitz MD, Haines DE, Haissaguerre M, Hindricks G, Iesaka Y, Jackman W, Jalife J, Jais P, Kalman J, Keane D, Kim YH, Kirchhof P, Klein G, Kottkamp H, Kumagai K, Lindsay BD, Mansour M, Marchlinski FE, McCarthy PM, Mont JL, Morady F, Nademanee K, Nakagawa H, Natale A, Nattel S, Packer DL, Pappone C, Prystowsky E, Raviele A, Reddy V, Ruskin JN, Shemin RJ, Tsao HM, Wilber D. Heart Rhythm Society Task Force on Catheter and Surgical Ablation of Atrial Fibrillation. 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design: a report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation. Developed in partnership with the European Heart Rhythm Association (EHRA), a registered branch of the European Society of Cardiology (ESC) and the European Cardiac Arrhythmia Society (ECAS); and in collaboration with the American College of Cardiology (ACC), American Heart Association (AHA), the Asia Pacific Heart Rhythm Society (APHRS), and the Society of Thoracic Surgeons (STS). Endorsed by the governing bodies of the American College of Cardiology Foundation, the American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons, the Asia Pacific Heart Rhythm Society, and the Heart Rhythm Society. Heart Rhythm. 2012; 9:632–696.e21.
Article11. Cox JL, Boineau JP, Schuessler RB, Ferguson TB Jr, Cain ME, Lindsay BD, Corr PB, Kater KM, Lappas DG. Successful surgical treatment of atrial fibrillation: review and clinical update. JAMA. 1991; 266:1976–1980.12. Cox JL. The first Maze procedure. J Thorac Cardiovasc Surg. 2011; 141:1093–1097.
Article13. Cox JL, Schuessler RB, D'Agostino HJ Jr, Stone CM, Chang BC, Cain ME, Corr PB, Boineau JP. The surgical treatment of atrial fibrillation. III. Development of a definitive surgical procedure. J Thorac Cardiovasc Surg. 1991; 101:569–583.14. Castellá M, Garcia-Valentin A, Pereda D, Colli A, Martinez A, Martinez D, Ramirez J, Mulet J. Anatomic aspects of the atrioventricular junction influencing radiofrequency Cox maze IV procedures. J Thorac Cardiovasc Surg. 2008; 136:419–423.
Article15. Bum Kim J, Suk Moon J, Yun SC, Kee Kim W, Jung SH, Jung Choo S, Song H, Hyun Chung C, Won Lee J. Long-term outcomes of mechanical valve replacement in patients with atrial fibrillation: impact of the maze procedure. Circulation. 2012; 125:2071–2080.
Article16. Konings KT, Kirchhof CJ, Smeets JR, Wellens HJ, Penn OC, Allessie MA. High-density mapping of electrically induced atrial fibrillation in humans. Circulation. 1994; 89:1665–1680.
Article17. Moe GK, Rheinboldt WC, Abildskov JA. A computer model of atrial fibrillation. Am Heart J. 1964; 67:200–220.
Article18. Haïssaguerre M, Marcus FI, Fischer B, Clementy J. Radiofrequency catheter ablation in unusual mechanisms of atrial fibrillation: report of three cases. J Cardiovasc Electrophysiol. 1994; 5:743–751.
Article19. Jongbloed MR, Schalij MJ, Poelmann RE, Blom NA, Fekkes ML, Wang Z, Fishman GI, Gittenberger-De Groot AC. Embryonic conduction tissue: a spatial correlation with adult arrhythmogenic areas. J Cardiovasc Electrophysiol. 2004; 15:349–355.20. Zhou J, Scherlag BJ, Edwards J, Jackman WM, Lazzara R, Po SS. Gradients of atrial refractoriness and inducibility of atrial fibrillation due to stimulation of ganglionated plexi. J Cardiovasc Electrophysiol. 2007; 18:83–90.
Article21. Lee JW, Choo SJ, Kim KI, Song JK, Kang DH, Song JM, Song H, Lee SK, Song MG. Atrial fibrillation surgery simplified with cryoablation to improve left atrial function. Ann Thorac Surg. 2001; 72:1479–1483.
Article22. Kim JB, Bang JH, Jung SH, Choo SJ, Chung CH, Lee JW. Left atrial ablation versus biatrial ablation in the surgical treatment of atrial fibrillation. Ann Thorac Surg. 2011; 92:1397–1404.
Article23. Calò L, Lamberti F, Loricchio ML, De Ruvo E, Colivicchi F, Bianconi L, Pandozi C, Santini M. Left atrial ablation versus biatrial ablation for persistent and permanent atrial fibrillation: a prospective and randomized study. J Am Coll Cardiol. 2006; 47:2504–2512.
Article24. Scharf C, Veerareddy S, Ozaydin M, Chugh A, Hall B, Cheung P, Good E, Pelosi F Jr, Morady F, Oral H. Clinical significance of inducible atrial flutter during pulmonary vein isolation in pa tients with atrial fibrillation. J Am Coll Cardiol. 2004; 43:2057–2062.
Article25. Wolf RK, Schneeberger EW, Osterday R, Miller D, Merrill W, Flege JB Jr, Gillinov AM. Video-assisted bilateral pulmonary vein isolation and left atrial appendage exclusion for atrial fibrillation. J Thorac Cardiovasc Surg. 2005; 130:797–802.
Article26. Shinbane JS, Lesh MD, Stevenson WG, Klitzner TS, Natterson PD, Wiener I, Ursell PC, Saxon LA. Anatomic and electrophysiologic relation between the coronary sinus and mitral annulus: implications for ablation of left-sided accessory pathways. Am Heart J. 1998; 135:93–98.
Article27. Edgerton JR, Jackman WM, Mack MJ. A new epicardial lesion set for minimal access left atrial maze: the Dallas lesion set. Ann Thorac Surg. 2009; 88:1655–1657.
Article28. Sirak J, Jones D, Schwartzman D. The five-box thoracoscopic maze procedure. Ann Thorac Surg. 2010; 90:986–989.
Article29. Balkhy HH, Chapman PD, Arnsdorf SE. Minimally invasive atrial fibrillation ablation combined with a new technique for thoracoscopic stapling of the left atrial appendage: case report. Heart Surg Forum. 2004; 7:353–355.
Article30. Pak HN, Hwang C, Lim HE, Kim JS, Kim YH. Hybrid epicardial and endocardial ablation of persistent or permanent atrial fibrillation: a new approach for difficult cases. J Cardiovasc Electrophysiol. 2007; 18:917–923.
Article31. Krul SP, Driessen AH, van Boven WJ, Linnenbank AC, Geuzebroek GS, Jackman WM, Wilde AA, de Bakker JM, de Groot JR. Thoracoscopic video-assisted pulmonary vein antrum isolation, ganglionated plexus ablation, and periprocedural confirmation of ablation lesions: first results of a hybrid surgical-electrophysiological approach for atrial fibrillation. Circ Arrhythm Electrophysiol. 2011; 4:262–270.
Article32. Eguchi K, Ohtaki E, Matsumura T, Tanaka K, Tohbaru T, Iguchi N, Misu K, Asano R, Nagayama M, Sumiyoshi T, Kasegawa H, Hosoda S. Pre-operative atrial fibrillation as the key determinant of outcome of mitral valve repair for degenerative mitral regurgitation. Eur Heart J. 2005; 26:1866–1872.
Article33. Doukas G, Samani NJ, Alexiou C, Oc M, Chin DT, Stafford PG, Ng LL, Spyt TJ. Left atrial radiofrequency ablation during mitral valve surgery for continuous atrial fibrillation: a randomized controlled trial. JAMA. 2005; 294:2323–2329.
Article34. Deneke T, Khargi K, Grewe PH, Laczkovics A, von Dryander S, Lawo T, Muller KM, Lemke B. Efficacy of an additional MAZE procedure using cooled-tip radiofrequency ablation in patients with chronic atrial fibrillation and mitral valve disease: a randomized, prospective trial. Eur Heart J. 2002; 23:558–566.
Article35. Abreu Filho CA, Lisboa LA, Dallan LA, Spina GS, Grinberg M, Scanavacca M, Sosa EA, Ramires JA, Oliveira SA. Effectiveness of the maze procedure using cooled-tip radiofrequency ablation in patients with permanent atrial fibrillation and rheumatic mitral valve disease. Circulation. 2005; 112:9 Suppl. I20–I25.
Article36. Budera P, Straka Z, Osmancik P, Vanek T, Jelinek S, Hlavicka J, Fojt R, Cervinka P, Hulman M, Smid M, Maly M, Widimsky P. Comparison of cardiac surgery with left atrial surgical ablation vs. cardiac surgery without atrial ablation in patients with coronary and/or valvular heart disease plus atrial fibrillation: final results of the PRAGUE-12 randomized multicentre study. Eur Heart J. 2012; 33:2644–2652.
Article37. Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, Kim YH, Klein G, Natale A, Packer D, Skanes A, Ambrogi F, Biganzoli E. Updated worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circ Arrhythm Electrophysiol. 2010; 3:32–38.
Article38. Packer DL, Kowal RC, Wheelan KR, Irwin JM, Champagne J, Guerra PG, Dubuc M, Reddy V, Nelson L, Holcomb RG, Lehmann JW, Ruskin JN. STOP AF Cryoablation Investigators. Cryoballoon ablation of pulmonary veins for paroxysmal atrial fibrillation: first results of the North American Arctic Front (STOP AF) pivotal trial. J Am Coll Cardiol. 2013; 61:1713–1723.
Article39. Wilber DJ, Pappone C, Neuzil P, De Paola A, Marchlinski F, Natale A, Macle L, Daoud EG, Calkins H, Hall B, Reddy V, Augello G, Reynolds MR, Vinekar C, Liu CY, Berry SM, Berry DA. ThermoCool AF Trial Investigators. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA. 2010; 303:333–340.
Article40. Gammie JS, Haddad M, Milford-Beland S, Welke KF, Ferguson TB Jr, O'Brien SM, Griffith BP, Peterson ED. Atrial fibrillation correction surgery: lessons from the Society of Thoracic Surgeons National Cardiac Database. Ann Thorac Surg. 2008; 85:909–914.
Article41. Cheema A, Vasamreddy CR, Dalal D, Marine JE, Dong J, Henrikson CA, Spragg D, Cheng A, Nazarian S, Sinha S, Halperin H, Berger R, Calkins H. Long-term single procedure efficacy of catheter ablation of atrial fibrillation. J Interv Card Electrophysiol. 2006; 15:145–155.
Article
