J Korean Soc Spine Surg.
2003 Jun;10(2):90-96. 10.4184/jkss.2003.10.2.90.
Posterolateral Fusion for Unstable Thoracolumbar Junction
- Affiliations
-
- 1Department of Orthopedic Surgery, Fatima Hospital, Daegu, Korea. tjddlr@mdhouse.com
- KMID: 2003205
- DOI: http://doi.org/10.4184/jkss.2003.10.2.90
Abstract
- STUDY DESIGN: A retrospective study of patients with a posterolateral spinal fusion for an unstable thoracolumbar junction.
OBJECTIVES
To evaluate the efficacy of a posterolateral spinal fusion for an unstable thoracolumbar junction. SUMMARY OF LITERATURE REVIEW: Posterolateral spinal fusions are well documented for their efficacy in the lumbar and lumbosacral spine, and have also been applied to the thoracolumbar junction in the lumbar area. The thoracolumbar junction, however, is a little different from the lumbar spine, in its anatomical and biomechanical aspects, and posterolateral fusions have not been well evaluated in these respects.
MATERIALS AND METHODS
Fourteen consecutive patients, who had posterolateral spinal fusions, with instrumentation for an unstable condition, including T12-L1 segment, and followed for more than one year, were included. In 11 patients, all the fractures had been decompressed posteriorly, for degenerative conditions in 2, and for a neoplastic pathology in the other one. The radiographs concerning the lateral fusion mass were reviewed according to Lenke's classification, the change in the segmental sagittal angle of the fused segment and the fixation failure of the instrumentation. The medical records relating to the neurological recovery were reviewed using the modified Frankel grading, and the overall clinical results of treatment by the Kirkaldy-Willis criteria.
RESULTS
All patients disclosed big, bilateral and solid fusion masses, with the exception of one patient who revealed a big, solid fusion mass on one side, and small, thin fusion mass on the other. No patient revealed more than 3 degrees of mobility on flexion-extension lateral radiographs, any evidence of fixation failure of the instrumentation. The neurological recovery, by the modified Frankel grading system, showed an average 1.3 improvement. The clinical results were excellent in 6, good in 6 and fair in 2 patients, with no poor results.
CONCLUSIONS
A posterolateral spinal fusion can be effectively applied in an unstable thoracolumbar junction, such as in the lumbar and lumbosacral spine, provided there is precise preparation of the graft beds, enough bone grafts and correction of the excessive kyphotic angle by the compression fixation of the posterior instrumentation.
MeSH Terms
Figure
-
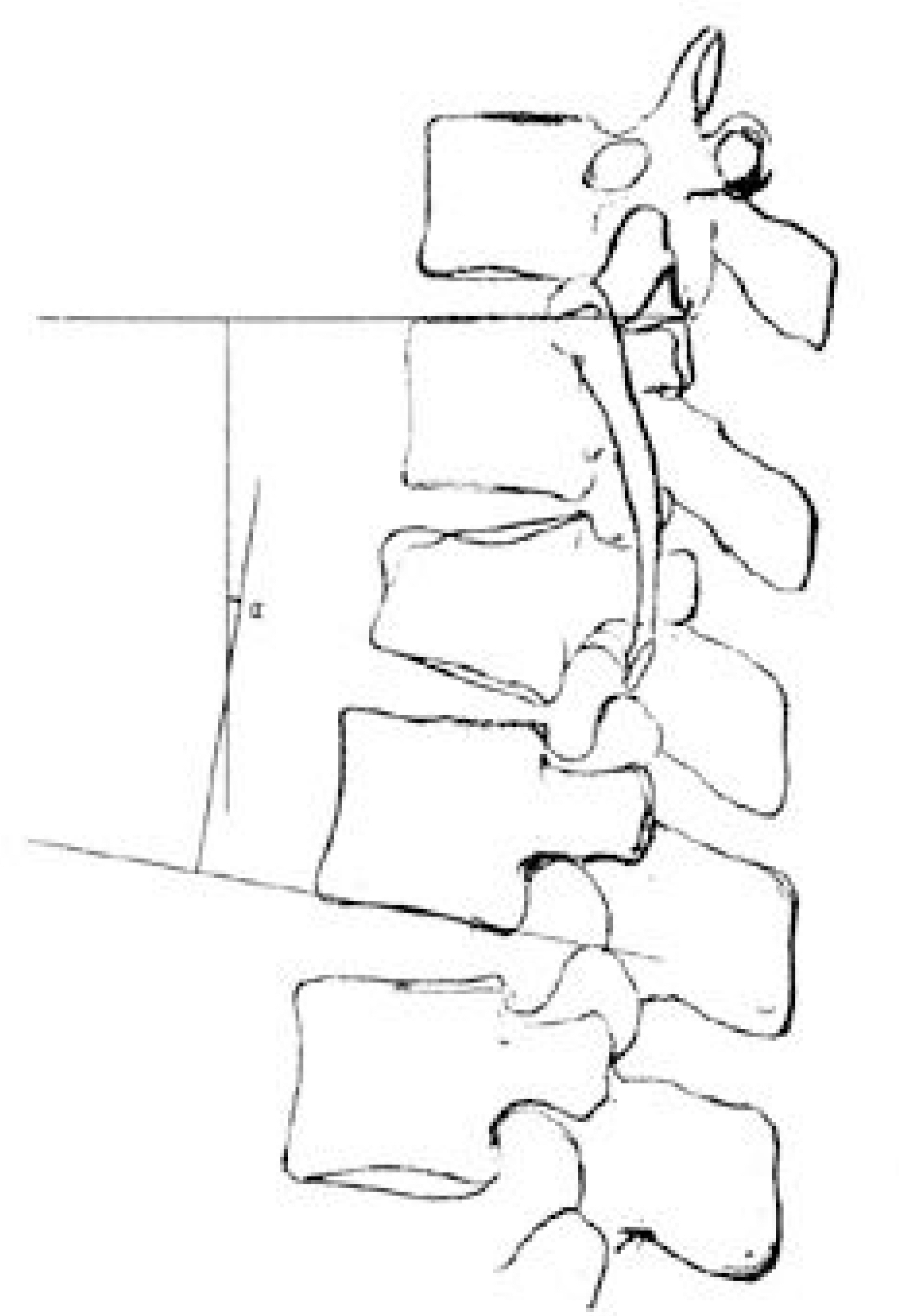
Fig. 1. Segmental sagittal angle of the fused segment. Fig. 1. Measured from the superior endplate of the most cranial vertebra to the inferior endplate of the most caudal vertebra in the fusion segment.

Fig. 2. A patient showing Lenke classification A. Fig. 1. Solid, big trabeculated fusions bilaterally.

Fig. 3. A patient showing Lenke classification B. Fig. 1. Solid, big fusion mass unilaterally with a small fusion mass on the contralateral aspect.

Fig. 4. The change of segmental sagittal angle of the fused segment on last follow-up flexion and extension view.
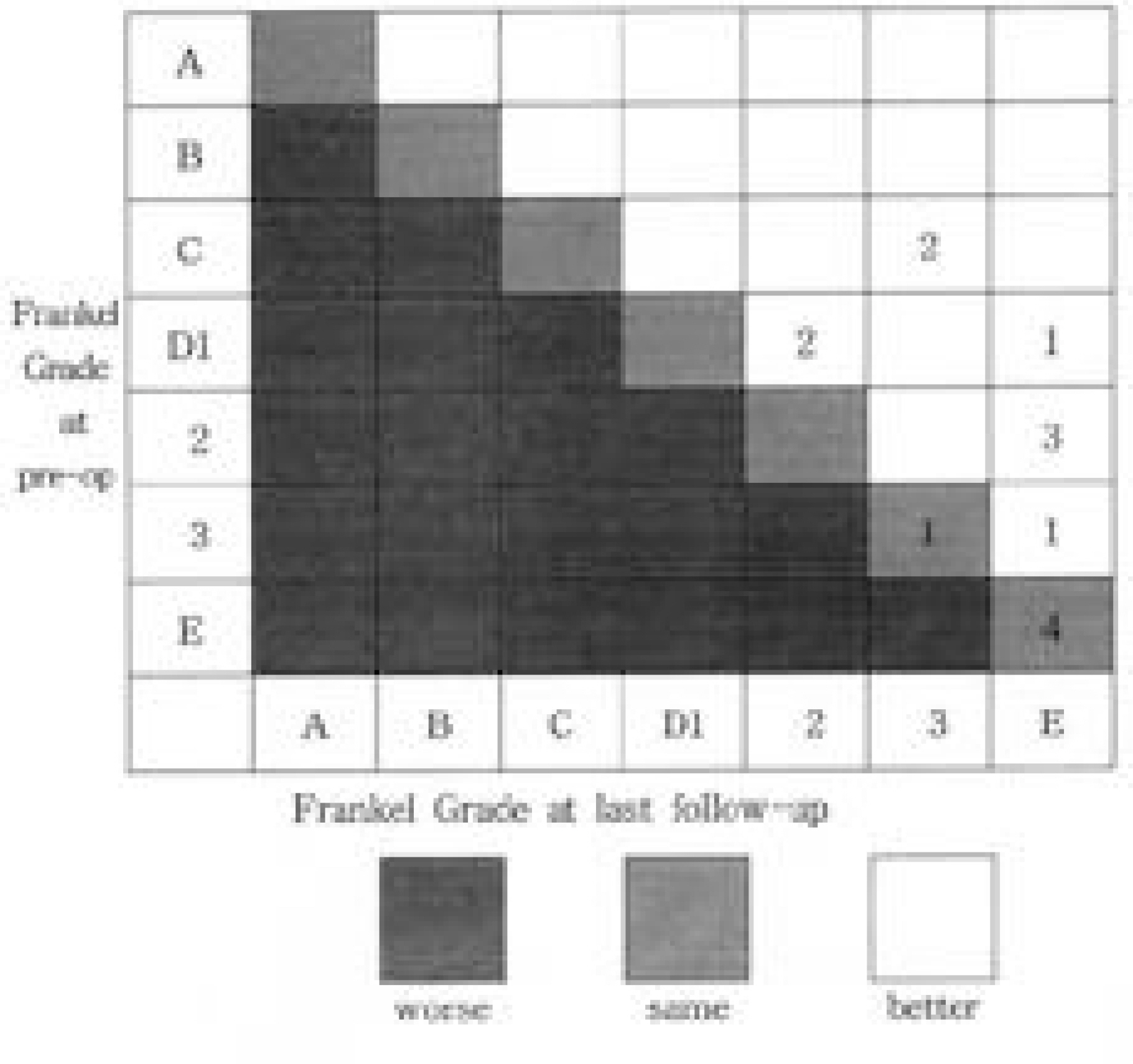
Fig. 5. Diagram showing change in modified Frankel grades between the preoperative status (vertical axis) and the status at last follow-up (horizontal axis)
Reference
-
01). Ahn JS. Biomechanics of lumbar spinal fusion. J Kor Spine Surg,. 7:126–132. 2000.02). Been HD. Anterior decompression and stabilization of thoracolumbar burst fractures by the use of the slot-zielke device. Spine,. 16:70–77. 1991.
Article03). Boucher M., Bhandari M., Kwok D. Health-related quality of life after short segment instrumentation of lum -bar burst fractures. J Spinal Disord,. 14:417–426. 2001.04). Bradford DS., Mcbride GG. Surgical management of thoracolumbar spine fractures with incomplete neuro -logic deficits. Clin Orthop,. 218:201–216. 1987.05). Cunningham BW., Polly DW Jr. The use of inter -body cage devices for spinal deformity: A biomechanical perspective. Clin Orthop,. 394:73–83. 2002.06). Denis F. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine,. 8:817–831. 1983.
Article07). Gaines RW Jr. The use of pedicle-screw internal fixation for the operative treatment of spinal disorders. J Bone Joint Surg Am,. 82:1458–1476. 2000.
Article08). Gaines RW Jr., Carson WL., Satterlee CC., Groh GI. Experimental evaluation of seven different spinal fracture internal fixation devices using nonfailure stability testing. Spine,. 16:902–909. 1991.
Article09). Goel VK., Gilbertson LG. Basic science of spinal instrumentation. Clin Orthop,. 335:10–31. 1997.
Article10). Herkowitz HN., Sidbu KS. Lumbar spine fusion in the treatment of degenerative conditions; current indications and recommendations. J Am Acad Orthop Surg,. 3:123–135. 1995.
Article11). Huler RJ. Thoracolumbar spine fracture. Frmoyer JW, editor. The adult spine-principles and practice. 2nd ed.Philadelphia: Lippincott-Raven;p. 1473. 1997.12). Kanayama M., Cunningham BW., Sefter JC., Goldstein JA., Stewart G., Kaneda K., McAfee PC. Does spinal instrumentation influence the healing process of postero -lateral spinal fusion ?; An in vivo animal model. Spine,. 24:1058–1065. 1999.13). Katonis PG., Kontakis GM., Loupasis GA., Aligizakis AC., Christoforakis JI andVelivassakis EG. Treatment of unstable thoracolumbar and lumbar spine injuries using Cotrel-Dubousset instrumentation. Spine,. 24:2352–2357. 1999.
Article14). Kirkaldy-Willis WH., Paine KWE., Cauchix J., Mclver G. Lumbar spinal stenosis. Clin Orthop,. 99:30–52. 1974.15). Knop C., Bastian L., Lange U., Oeser M., Zdichavsky M., Blauth M. Complications in surgical treatment of thoracolumbar injuries. Eur Spine J,. 11:214–226. 2002.
Article16). Lee CK., Langrana NA. Lumbosacral spinal fusion: a biomechanical study. Spine,. 9:574–581. 1984.
Article17). Lee CS., Choi JS., Kim YC., Seo SS., Ahn KC., Jeon JW., Shin JH., Na CO. Survival analysis of posterior short fusion in thoracolumbar fracture; Significance of load -sharing score and bone mineral density. J Kor Spine Surg,. 8:113–119. 2001.18). Lenke LG., Bridwell KH., Bullis D., Baldus RRBC., Schoenecker PL. Results of in situ fusion for isthmic spondylolisthesis. J Spinal Disord,. 5:433–442. 1992.
Article19). Macnab I., Dall D. The blood supply of the lumbar spine and its application to the technique of intertrans -verse lumbar fusion. J Bone Joint Surg,. 53B:628–638. 1971.20). Oda T., Panjabi NM. Pedicle screw adjustments affect stability of thoracolumbar burst fracture. Spine,. 26:2328–2333. 2001.
Article21). Park BM., Kang ES., Hwang SK. Study on postero -lateral fusion of lumbar spine. J Korean Orthop Assoc,. 14:482–488. 1979.22). Parker JW., Lane JR., Karaikovic EE., Gaines RW. Successful short-segment i-nstrumentation and fusion for thoracolumbar spine fractures. Spine,. 25:1157–1169. 2000.
Article23). Schnee CL., Ansell LV. Selection criteria and out -come of operative approaches for thoracolumbar burst fractures with and without neurological deficit. J Neuro -surg,. 86:48–55. 1997.24). Watkins MB. Posterolateral fusion of the lumbar and lumbosacral spine. J Bone Joint Surg,. 35A:1014. 1953.
Article25). You JW. Posterolateral fusion of lumbar spine. J Kor Spine Surg,. 7:169–175. 2000.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anterior and Posterior Stabilization by One Stage Posterolateral Approach in the Unstable Fracture of Thoracolumbar and Lumbar Spine
- Comparison of Posterior Fixation Alone and Supplementation with Posterolateral Fusion in Thoracolumbar Burst Fractures
- The Posterolateral Decompression for Burst Fracture in the Thoracolumbar Spine
- Clinical Results of Segmental spinal instrumentation in Unstable Fracture and Fracture - Dislocation of the Thoracolumbar Spine
- Clinical Analysis of Anterior Interbody Fusion Using Kaneda Device in Unstable Thoracolumbar Spinal Lesions(Long Term Follow-up Results)
