Biceps Femoris Tendon and Lateral Collateral Ligament: Analysis of Insertion Pattern Using MRI
- Affiliations
-
- 1Department of Radiology, Kyung Hee University Hospital, Kyung Hee University, Seoul, Korea.
- 2Department of Radiology, Kyung Hee University Hospital, Seoul, Korea. t2star@khu.ac.kr
- 3Department of Radiology, Kyung Hee University Hospital at Gandong, Seoul, Korea.
- 4Department of Radiology, Jeju National University Hospital, Jeju-do, Korea.
- KMID: 1999922
- DOI: http://doi.org/10.13104/jksmrm.2014.18.3.225
Abstract
- PURPOSE
The biceps femoris tendon (BFT) and lateral collateral ligament (LCL) in the knee were formerly known to form a conjoined tendon at the fibular attachment site. However, the BFT and LCL are attached into the fibular head in various patterns. We classified insertion patterns of the BFT and LCL using MR imaging, and analyzed whether the LCL attaches to the fibular head or not.
MATERIALS AND METHODS
A total of 494 consecutive knee MRIs of 470 patients taken between July 2012 and December 2012 were retrospectively reviewed. There were 224 males and 246 females, and patient age varied from 10 to 88 (mean, 48.6). The exclusion criteria were previous surgery and poor image quality. Using 3T fat-suppressed proton density-weighted axial images, the fibular insertion patterns of the BFT and LCL were classified into following types: type I (the LCL passes between the anterior arm and direct arm of the BFT's long head), type II (the LCL joins with anterior arm of the long head of the BFT), type III (the BFT and LCL join to form a conjoined tendon), type IV (the LCL passes laterally around the anterior margin of the BFT), and type V (the LCL passes posteriorly to the direct arm of the BFT's long head).
RESULTS
Among the 494 cases of the knee MRI, there were 433 (87.65%) type I cases, 21 (4.25%) type II cases, 2 (0.4%) type III cases, 16 (3.23%) type IV cases, and 22 (4.45%) type V cases. There were 26 cases (5.26%) in which the LCL and BFT were not attached into the fibular head.
CONCLUSION
The fibular attachment pattern of the BFT and LCL shows diverse types in MR imaging. The LCL does not adhere to the head in some patients.
MeSH Terms
Figure
-
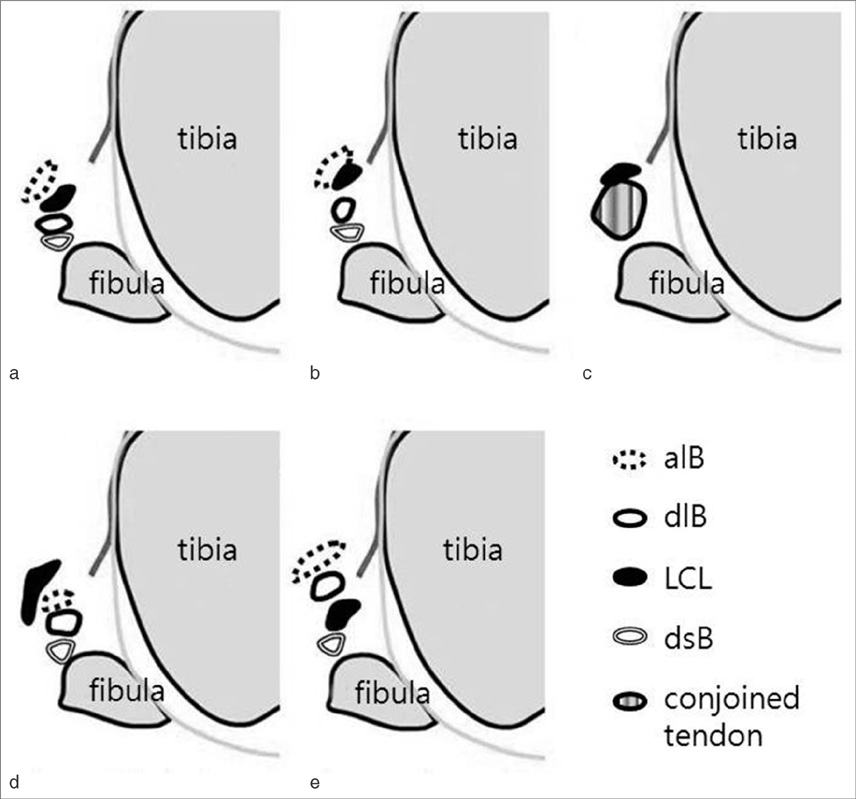
Fig. 1 Fibular insertion of the BFT and LCL, alB: anterior arm of the BFT's long head, dlB: direct arm of the BFT's long head, dsB: direct arm of the BFT's short head. (a) Type I, the LCL passes between the anterior arm and direct arm of the BFT's long head. (b) Type II, LCL joins with the anterior arm of the BFT's long head. (c) Type III, the BFT and LCL join to form a conjoined tendon. (d) Type IV, the LCL passes laterally around the anterior margin of the BFT. (e) Type V, the LCL passes posteriorly to the direct arm of the BFT's long head.
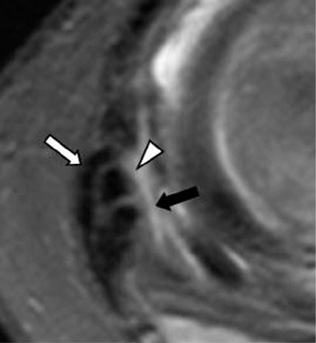
Fig. 2 28-years-old female, type I. 3T proton density fat suppressed axial image (TR/TE, 4036/20). LCL (arrowhead) passes between the anterior arm (open arrow) and direct arm (solid arrow) of the BFT's long head.

Fig. 3 12-years-old male, type II. (a, b) 3T proton density fat suppressed axial image (TR/TE, 4036/20). The anterior arm (open arrow) of the BFT's long head joins with LCL (arrowhead). The solid arrow indicates the direct arm of the BFT's long head.

Fig. 4 52-years-old male, type III. (a) 3T proton density fat suppressed axial image (TR/TE, 4036/20). BFT (open arrow) is not divided into separate arms, and forms a fused mass. The arrowhead indicates the LCL. (b) In a lower level, BFT and LCL joins and forms a conjoined tendon (stripe arrow).

Fig. 5 61-years-old male, type IV. 3T proton density fat suppressed axial image (TR/TE, 4036/20). LCL (arrowhead) passes laterally to the anterior arm (open arrow) of BFT. The solid arrow indicates the direct arm of long head of BFT. Stripe arrow indicates fibula.
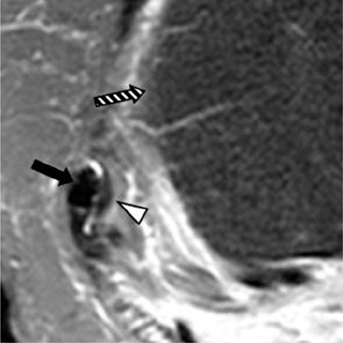
Fig. 6 64-years-old female, type V. 3T proton density fat suppressed axial image (TR/TE, 4036/20). LCL (arrowhead) passes posteriorly to the direct arm (solid arrow) of long head of BFT. Stripe arrow indicates tibia.
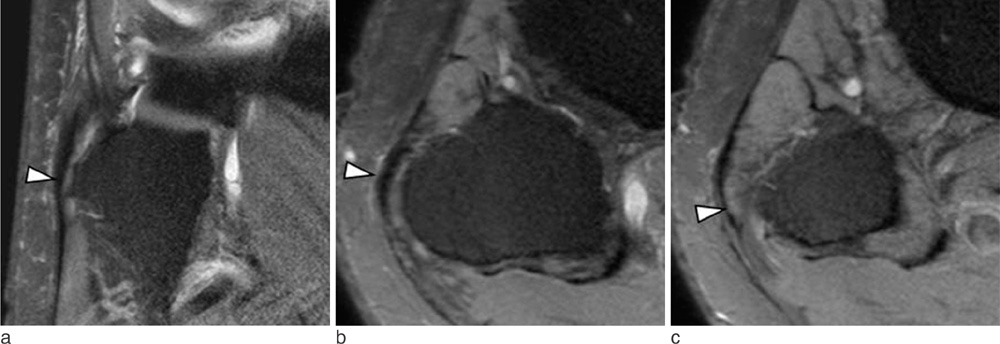
Fig. 7 28-years-old male patient without fibular insertion of the LCL. (a) Proton density (PD) fat suppressed coronal image (TR/TE, 5000/30) and (b) axial image show LCL (arrowhead) passing the fibular head without attachment. (c) In a lower level, axial image show LCL (arrowhead) passing the fibular head laterally in an aponeurosis form.
Reference
-
1. Recondo JA, Salvador E, Villanúa JA, Barrera MC, Gervás C, Alústiza JM. Lateral stabilizing structures of the knee: functional anatomy and injuries assessed with MR imaging. Radiographics. 2000; 20:S91–S102.2. Sneath RS. The insertion of the biceps femoris. J Anat. 1955; 89:550–553.3. Terry GC, LaPrade RF. The biceps femoris muscle complex at the knee. Its anatomy and injury patterns associated with acute anterolateral-anteromedial rotatory instability. Am J Sports Med. 1996; 24:2–8.4. Pereira ER, Ryu KN, Ahn JM, Kayser F, Bielecki D, Resnick D. Evaluation of the anterior cruciate ligament of the knee: comparison between partial flexion true sagittal and extension sagittal oblique positions during MR imaging. Clin Radiol. 1998; 53:574–578.5. Munshi M, Pretterklieber ML, Kwak S, Antonio GE, Trudell DJ, Resnick D. MR imaging, MR arthrography, and specimen correlation of the posterolateral corner of the knee: an anatomic study. AJR Am J Roentgenol. 2003; 180:1095–1110.6. DeLee JC, Riley MB, Rockwood CA Jr. Acute posterolateral rotatory instability of the knee. Am J Sports Med. 1983; 11:199–207.7. Tubbs RS, Caycedo FJ, Oakes WJ, Salter EG. Descriptive anatomy of the insertion of the biceps femoris muscle. Clin Anat. 2006; 19:517–521.8. Espregueira-Mendes , da Silva MV. Anatomy of the lateral collateral ligament: a cadaver and histological study. Knee Surg Sports Traumatol Arthrosc. 2006; 14:221–228.9. Solomon LB, Stevenson AW. Tibial insertion of the biceps femoris tendon: anatomical and radiological description of an anatomical variant. Clin Anat. 2008; 21:802–804.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anomalous Biceps Femoris Tendon Insertion Leading to a Snapping Knee in a Young Male
- Patellar Tendon Rupture associated with Rupture of Anterior Cruciate Ligament, Both Collateral Ligoments, and Lateral Meniscus: A Case Report
- Magnetic Resonance Imaging for the Evaluation of Acute Posterolateral Complex Injuries of the Knee
- Calcification of the Lateral Collateral Ligament of the Knee: A Case Report
- Which Approach Is Most Optimal for Needle Electromyographic Examination of the Biceps Femoris Short Head: Medial or Lateral?
