Preliminary Results for Continence Recovery after Intrafascial Extraperitoneal Laparoscopic Radical Prostatectomy
- Affiliations
-
- 1Department of Urology, Pusan National University Hospital, Busan, Korea. hongkooha@pusan.ac.kr
- KMID: 1988728
- DOI: http://doi.org/10.4111/kju.2012.53.12.836
Abstract
- PURPOSE
We present our initial experience and surgical outcomes for the most recent refinement of bilateral intrafascial nerve-sparing extraperitoneal laparoscopic radical prostatectomy (nsELRP).
MATERIALS AND METHODS
Among 62 patients who underwent laparoscopic radical prostatectomy, 50 patients underwent intrafascial nsELRP by a single surgeon at Pusan National University Hospital from November 2011 to April 2012. As part of the intrafascial technique, the dissection plane is directly on the prostatic capsule to preserve most of the periprostatic fascia containing small vessels and nerves, endopelvic fascia, neurovascular bundle, and puboprostatic ligament. Postoperative continence recovery was established by daily consumption of pads. Follow-up was done at 2 weeks, 6 weeks, and 3 months after surgery.
RESULTS
The patients' mean age was 66.5+/-6.2 years. The mean operation time and mean blood loss were 149.3+/-28.1 minutes and 155.4+/-168.1 ml, respectively. The mean hospitalization time and mean catheterization time were 6.3+/-5.1 days and 5.5+/-4.7 days, respectively. Two weeks after the operation, a total of 14 patients (28.0%) were pad-free but the other incontinent patient group used on average 2.3 pads per day. After 6 weeks, 35 patients (70.0%) achieved pad-free status and 7 patients (14.0%) required more than 2 pads per day. At 3 months after surgery, a total of 31 patients were available for follow-up, and 26 patients (83.9%) were pad-free.
CONCLUSIONS
Compared with conventional laparoscopic prostatectomy, the intrafascial nsELRP procedure enables the preservation of periprostatic structures that are essential to the recovery of surgical structures related to continence. As a result, early postoperative continence can be achieved.
Keyword
MeSH Terms
Figure
-

FIG. 1 Initial approach for intrafascial nerve-sparing extraperitoneal laparoscopic radical prostatectomy. Incision is made medial to the puboprostatic ligament. PPL, puboprostatic ligament; P, prostate; Bl, bladder; Ef, endopelvic fascia.

FIG. 2 Prostatic pedicle dissection and sparing of the neurovascular bundles. Both anterior and posterior neurovascular bundles were preserved by using cold scissors. P, prostate; aNVB, accessory neurovascular bundle; pNVB, predominant neurovascular bundle.
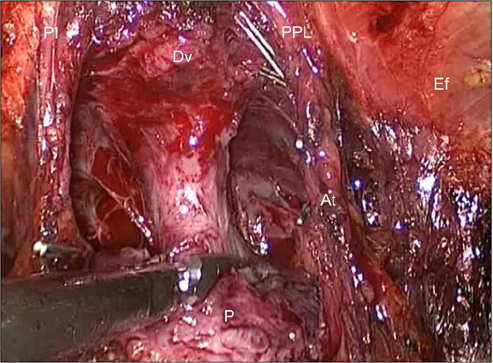
FIG. 3 Dissection of the prostate apex and urethra. Urethral dissection was performed proximally very close to the prostate to preserve urethral length. We did not ligate the deep dorsal venous plexus. The endopelvic fascia, which envelops the levator ani muscle, was preserved during surgery and the longer urethra was preserved. Both puboprostatic ligaments and arcuous tendinosus were also preserved. Dv, deep dorsal venous plexus; U, urethra; P, prostate; Ef, endopelvic fascia; PPL, puboprostatic ligament; At, arcuous tendinosus.
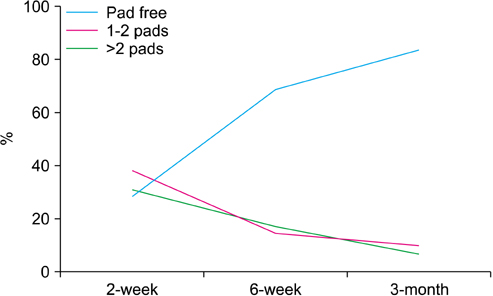
FIG. 4 Continence rates after intrafascial nerve-sparing extraperitoneal laparoscopic radical prostatectomy.
Cited by 1 articles
-
Learning Curve of Robot-Assisted Laparoscopic Radical Prostatectomy for a Single Experienced Surgeon: Comparison with Simultaneous Laparoscopic Radical Prostatectomy
Ja Yoon Ku, Hong Koo Ha
World J Mens Health. 2015;33(1):30-35. doi: 10.5534/wjmh.2015.33.1.30.
Reference
-
1. Anastasiadis AG, Salomon L, Katz R, Hoznek A, Chopin D, Abbou CC. Radical retropubic versus laparoscopic prostatectomy: a prospective comparison of functional outcome. Urology. 2003. 62:292–297.2. Guillonneau B, el-Fettouh H, Baumert H, Cathelineau X, Doublet JD, Fromont G, et al. Laparoscopic radical prostatectomy: oncological evaluation after 1,000 cases a Montsouris Institute. J Urol. 2003. 169:1261–1266.3. Stolzenburg JU, Do M, Pfeiffer H, Konig F, Aedtner B, Dorschner W. The endoscopic extraperitoneal radical prostatectomy (EERPE): technique and initial experience. World J Urol. 2002. 20:48–55.4. Ficarra V, Novara G, Artibani W, Cestari A, Galfano A, Graefen M, et al. Retropubic, laparoscopic, and robot-assisted radical prostatectomy: a systematic review and cumulative analysis of comparative studies. Eur Urol. 2009. 55:1037–1063.5. Stolzenburg JU, Liatsikos EN, Rabenalt R, Do M, Sakelaropoulos G, Horn LC, et al. Nerve sparing endoscopic extraperitoneal radical prostatectomy: effect of puboprostatic ligament preservation on early continence and positive margins. Eur Urol. 2006. 49:103–111.6. Stolzenburg JU, Rabenalt R, Tannapfel A, Liatsikos EN. Intrafascial nerve-sparing endoscopic extraperitoneal radical prostatectomy. Urology. 2006. 67:17–21.7. Salomon L, Sebe P, De la Taille A, Vordos D, Hoznek A, Yiou R, et al. Open versus laparoscopic radical prostatectomy: part I. BJU Int. 2004. 94:238–243.8. Salomon L, Sebe P, De la Taille A, Vordos D, Hoznek A, Yiou R, et al. Open versus laparoscopic radical prostatectomy: Part II. BJU Int. 2004. 94:244–250.9. Thompson I, Thrasher JB, Aus G, Burnett AL, Canby-Hagino ED, Cookson MS, et al. Guideline for the management of clinically localized prostate cancer: 2007 update. J Urol. 2007. 177:2106–2131.10. Myers RP. Practical surgical anatomy for radical prostatectomy. Urol Clin North Am. 2001. 28:473–490.11. Myers RP. Detrusor apron, associated vascular plexus, and avascular plane: relevance to radical retropubic prostatectomy--anatomic and surgical commentary. Urology. 2002. 59:472–479.12. Takenaka A, Hara R, Soga H, Murakami G, Fujisawa M. A novel technique for approaching the endopelvic fascia in retropubic radical prostatectomy, based on an anatomical study of fixed and fresh cadavers. BJU Int. 2005. 95:766–771.13. Savera AT, Kaul S, Badani K, Stark AT, Shah NL, Menon M. Robotic radical prostatectomy with the "Veil of Aphrodite" technique: histologic evidence of enhanced nerve sparing. Eur Urol. 2006. 49:1065–1073.14. Kiyoshima K, Yokomizo A, Yoshida T, Tomita K, Yonemasu H, Nakamura M, et al. Anatomical features of periprostatic tissue and its surroundings: a histological analysis of 79 radical retropubic prostatectomy specimens. Jpn J Clin Oncol. 2004. 34:463–468.15. Steiner MS. The puboprostatic ligament and the male urethral suspensory mechanism: an anatomic study. Urology. 1994. 44:530–534.16. Presti JC Jr, Schmidt RA, Narayan PA, Carroll PR, Tanagho EA. Pathophysiology of urinary incontinence after radical prostatectomy. J Urol. 1990. 143:975–978.17. Poore RE, McCullough DL, Jarow JP. Puboprostatic ligament sparing improves urinary continence after radical retropubic prostatectomy. Urology. 1998. 51:67–72.18. Deliveliotis C, Protogerou V, Alargof E, Varkarakis J. Radical prostatectomy: bladder neck preservation and puboprostatic ligament sparing: effects on continence and positive margins. Urology. 2002. 60:855–858.19. Burnett AL, Mostwin JL. In situ anatomical study of the male urethral sphincteric complex: relevance to continence preservation following major pelvic surgery. J Urol. 1998. 160:1301–1306.20. Graefen M, Walz J, Huland H. Open retropubic nerve-sparing radical prostatectomy. Eur Urol. 2006. 49:38–48.21. Tewari AK, Bigelow K, Rao S, Takenaka A, El-Tabi N, Te A, et al. Anatomic restoration technique of continence mechanism and preservation of puboprostatic collar: a novel modification to achieve early urinary continence in men undergoing robotic prostatectomy. Urology. 2007. 69:726–731.22. Stolzenburg JU, Rabenalt R, Do M, Schwalenberg T, Winkler M, Dietel A, et al. Intrafascial nerve-sparing endoscopic extraperitoneal radical prostatectomy. Eur Urol. 2008. 53:931–940.23. Albers DD, Faulkner KK, Cheatham WN, Elledge EF, Coalson RE. Surgical anatomy of the pubovesical (puboprostatic) ligaments. J Urol. 1973. 109:388–392.24. Rocco B, Cozzi G, Spinelli MG, Coelho RF, Patel VR, Tewari A, et al. Posterior musculofascial reconstruction after radical prostatectomy: a systematic review of the literature. Eur Urol. 2012. 62:779–790.25. Hurtes X, Roupret M, Vaessen C, Pereira H, Faivre d'Arcier B, Cormier L, et al. Anterior suspension combined with posterior reconstruction during robot-assisted laparoscopic prostatectomy improves early return of urinary continence: a prospective randomized multicentre trial. BJU Int. 2012. 110:875–883.26. Cambio AJ, Evans CP. Minimising postoperative incontinence following radical prostatectomy: considerations and evidence. Eur Urol. 2006. 50:903–913.27. Sievert KD, Hennenlotter J, Laible I, Amend B, Schilling D, Anastasiadis A, et al. The periprostatic autonomic nerves: bundle or layer? Eur Urol. 2008. 54:1109–1116.28. Ganzer R, Blana A, Gaumann A, Stolzenburg JU, Rabenalt R, Bach T, et al. Topographical anatomy of periprostatic and capsular nerves: quantification and computerised planimetry. Eur Urol. 2008. 54:353–360.29. Costello AJ, Brooks M, Cole OJ. Anatomical studies of the neurovascular bundle and cavernosal nerves. BJU Int. 2004. 94:1071–1076.30. Walsh PC. Anatomic radical prostatectomy: evolution of the surgical technique. J Urol. 1998. 160(6 Pt 2):2418–2424.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Extraperitoneal Laparoscopic Radical Prostatectomy: Initial Experience
- The Surgical Procedure Is the Most Important Factor Affecting Continence Recovery after Laparoscopic Radical Prostatectomy
- Extraperitoneal Laparoscopic Radical Prostatectomy: Clinical Experience and Learning Curve with 103 Cases
- Laparoscopic Simple Prostatectomy
- Effect of Posterior Urethral Reconstruction (PUR) in Early Recovery of Urinary Continence after Robotic-Assisted Radical Prostatectomy
