Tricuspid Valvular Myxoma: Unusual Case of Tricuspid Valve Myxoma Mimicking Thrombus after Pulmonary Artery Embolectomy and Tricuspid Annuloplasty in Pulmonary Thromboembolism Patient
- Affiliations
-
- 1Department of Cardiology, Inje University Ilsan Paik Hospital, Goyang, Korea. mdksu@paik.ac.kr
- 2Department of Thoracic Surgery, Inje University Ilsan Paik Hospital, Goyang, Korea.
- 3Department of Pathology, Inje University Ilsan Paik Hospital, Goyang, Korea.
- KMID: 1980385
- DOI: http://doi.org/10.4250/jcu.2011.19.4.207
Abstract
- A 55-year-old man with massive pulmonary thromboembolism underwent thrombolysis, pulmonary artery embolectomy and tricuspid annuloplasty. Nine months later, a mobile echogenic intra-cardiac mass was found in the tricuspid valve. Because the patient had undergone annuloplasty, thrombosis was suspected as the most likely diagnosis and thrombolytic therapy was instituted. However, the size of the cardiac mass did not change and after surgical excision the mass was found to be a myxoma. Cardiac valvular tumors are uncommon and when they occur they are usually slow growing fibroelastomas. In this case, the rapid growing cardiac myxoma on the tricuspid valve was found after the occurrence of pulmonary thromboembolism. To our knowledge, this is first reported case of tricuspid valve myxoma in Korea.
MeSH Terms
Figure
-
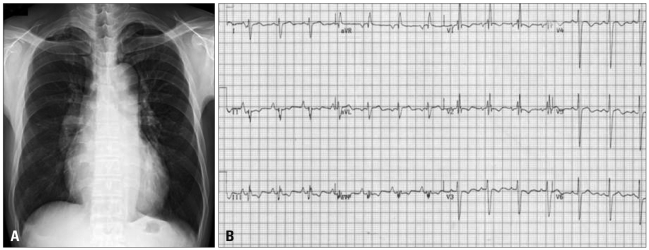
Fig. 1 A: Chest X-ray showed cardiomegaly with right atrial enlargement and a prominent pulmonary trunk. B: Electrocardiogram showed characteristic features of RV strain with prominent S wave in lead I, Q wave in lead III, with T-wave inversion in lead III. RV: right ventricle.
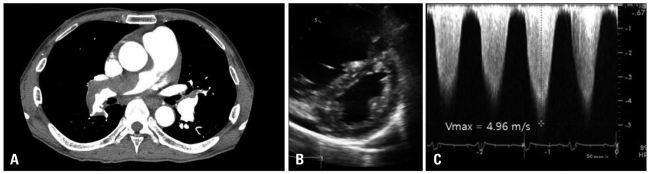
Fig. 2 A: Chest CT scanning detected a large thrombus in the right pulmonary artery. B: D-shaped LV was shown. C: Vmax was 4.96 m/s. Estimated right ventricular systolic pressure was 119 mm Hg (assumed right atrial pressure = 20 mm Hg, inferior vena cava dilatation and plethora was found). LV: left ventricle.
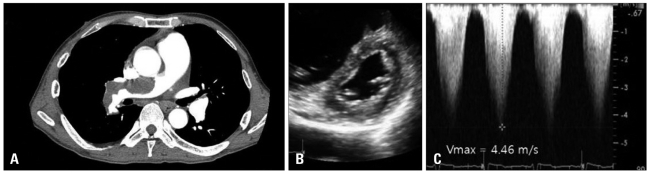
Fig. 3 A: A second computed tomogram showed a partially resolved multifocal extensive pulmonary thrombus. B: D-shaped LV remained after thrombolysis. C: Vmax was 4.46 m/s. After thrombolysis, estimated right ventricular systolic pressure was slightly reduced. LV: left ventricle.
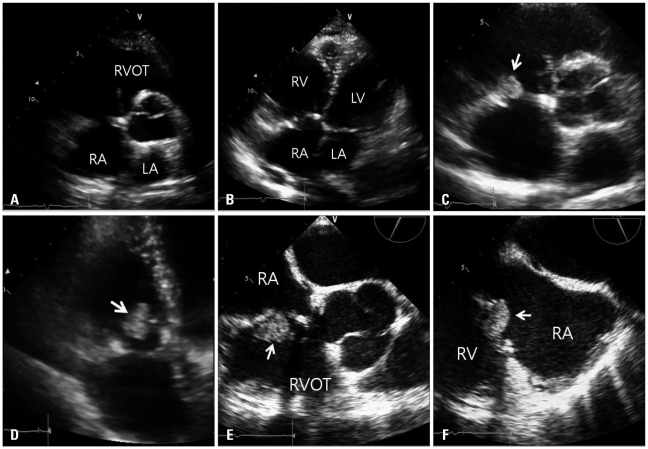
Fig. 4 A and B: Parasternal short axis view and apical four-chamber view. There was no visible mass in the immediate postoperative image. C and D: Parasternal short axis view and apical four-chamber view. There was a visible mass (arrow) with stalk 9 months later. E and F: Mid-esophageal RV inflow-outflow view in 64 degrees and mid-esophageal RV inflow view in 116 degrees. An intracardiac mass (arrow) was obvious (size: 2.2 × 1.5 cm2). After the 5th day of thrombolysis, the mass size remained unchanged. RA: right atrium, RV: right ventricle, RVOT: right ventricular outflow track, LA: left atrium, LV: left ventricle.
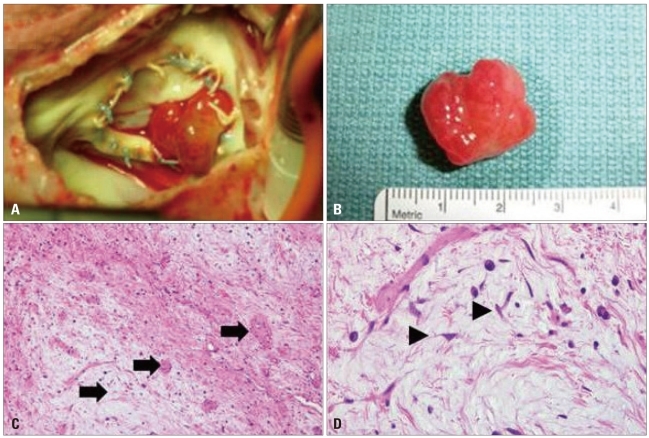
Fig. 5 A: After right atrial opening, photograph showed a polypoid mass attached between annulus and tricuspid valve. B: After excision, mass size was similar to echocardiographically measured size (resected tumor size was approximately 2.5 × 1.5 cm2). C: Histological findings with Hematoxylin-Eosin staining. Histological examination of the mass revealed that it was composed of scattered small oval or stellate cells with abundant myxoid matrix, consistent with a diagnosis of nonmalignant cardiac myxoma. The tumor was hypocellular with prominent myxoid stroma and thick walled blood vessels (arrows, × 100). D: The tumor cells were elongated or stellate (arrowheads). They had round to elongated nuclei and eosinophilic cytoplasm. Lymphoplasma cells and histiocytes are present (× 400).
Reference
-
1. 2009 Training program for authenticated echocardiographist [Internet]. Korean Society of Echocardiography. 2009. cited 2011 Feb 21. Available from: http://www.ksecho.org/infomation/contents/notice126/11_1.pdf.2. Pierre-Justin G, Pierard LA. Management of mobile right heart thrombi: a prospective series. Int J Cardiol. 2005; 99:381–388. PMID: 15771917.3. Piazza G, Goldhaber SZ. Fibrinolysis for acute pulmonary embolism. Vasc Med. 2010; 15:419–428. PMID: 20926501.4. Porath A, Avnun L, Hirsch M, Ovsyshcher I. Right atrial thrombus and recurrent pulmonary emboli secondary to permanent cardiac pacing--a case report and short review of literature. Angiology. 1987; 38:627–630. PMID: 3631647.5. Mügge A, Gulba DC, Jost S, Daniel WG. Dissolution of a right atrial thrombus attached to pacemaker electrodes: usefulness of recombinant tissuetype plasminogen activator. Am Heart J. 1990; 119:1437–1439. PMID: 2112880.6. Reynen K. Cardiac myxomas. N Engl J Med. 1995; 333:1610–1617. PMID: 7477198.7. Graça A, Nunes R, Costeira A, Almeida J, Bastos P. Cardiac papillary fibroelastoma of a mitral valve chordae revealed by stroke. Rev Port Cardiol. 1999; 18:937–939. PMID: 10590658.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Right Ventricular Myxoma Which Attached to the Tricuspid Valve: Sliding Tricuspid Valvuloplasty
- Left Atrial Myxoma Associated with Mitral Regurgitation and Coronary Artery Disease
- Pulmonary Thromboembolism and Infarction Caused by Right-Sided Infective Endocarditis in a Patient with Ventricular Septal Defect
- Tricuspid Valve Repair for Tricuspid Valve Insufficiency Following a Cardiac Stab Injury
- A case of congenital tricuspid stenosis
