Primary Endobronchial Leiomyoma Combined with Uterine Leiomyoma
- Affiliations
-
- 1Department of Internal medicine, School of Medicine, Chonnam National University, Gwangju, Korea. cyberkks@chonnam.ac.kr
- 2Department of Obstetrics and Gynecology, School of Medicine, Chonnam National University, Gwangju, Korea.
- 3Department of Thoracic and Cardiovascular Surgery, School of Medicine, Chonnam National University, Gwangju, Korea.
- KMID: 1970256
- DOI: http://doi.org/10.4046/trd.2006.61.5.490
Abstract
- Leiomyoma of the bronchus is a very rare benign tumor of the lung. Most endobronchial leiomyomas occur as secondary foci of primary uterine leiomyoma. We herein report a case with endobronchial tumor that had a different pathology from a primary resected uterine leiomyoma and was therefor considered a primary endobronchial leiomyoma. A 51-year-old woman with a history of uterine myoma presented with productive cough and fever. Bronchoscopy revealed a lightly yellow colored mass lesion that totally obstructed the orifice of the left lower lobe of the lung. The diagnosis of leiomyoma was made by histological examination of the obtained specimen. We considered the possibility of a benign metastasizing pulmonary leiomyoma. For treatment and differential diagnosis, a left lower lobe lobectomy of the lung and total hysterectomy with bilateral salphingooopherectomy were performed. The differences between lung and uterine lesions were confirmed by morphologic finding and immunohistochemical staining. The pathological diagnosis was primary endobronchial leiomyoma combined with uterine myoma.
MeSH Terms
Figure
-
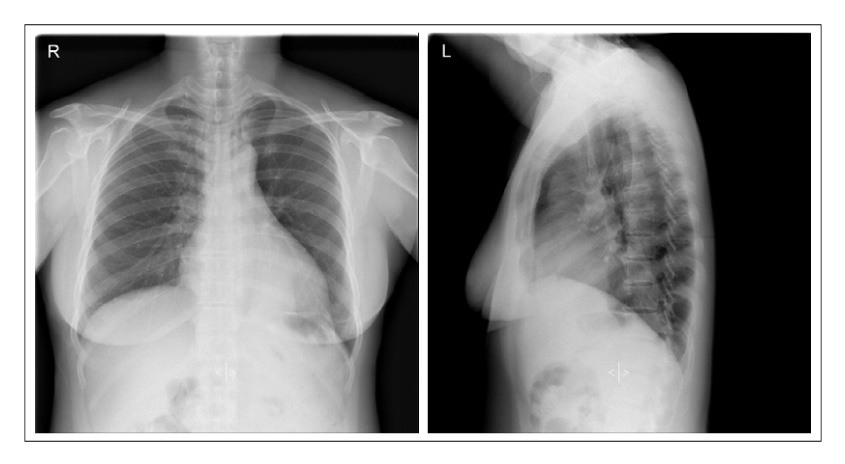
Figure 1 Chest radiography showed mass like lesion with passive atelectasis in left lower lobe.
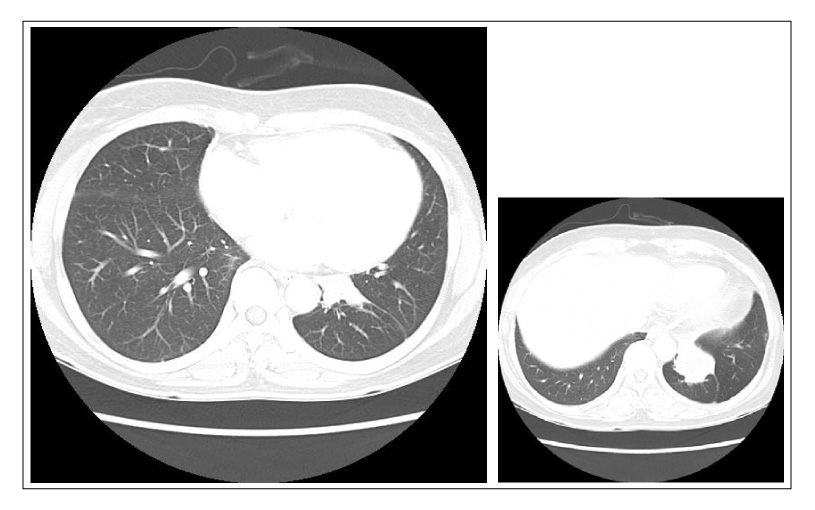
Figure 2 Chest CT scan reveals about 4.8×3.8 cm sized enhancing mass in left lower lobe.
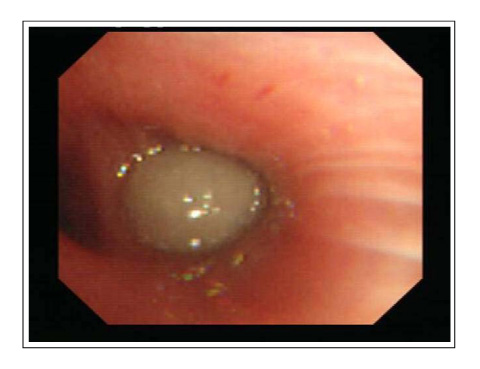
Figure 3 Bronchoscopy showed yellowish, round, hard mass, completely obstructing left lower lobe bronchus.
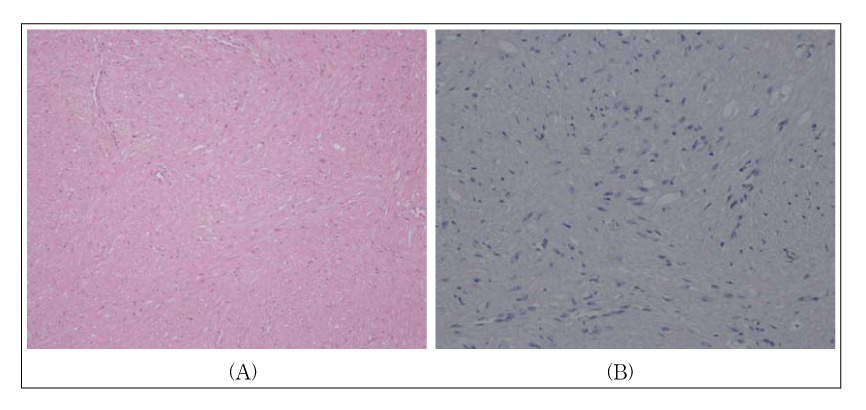
Figure 4 (A) Microscopic finding of the resected pulmonary mass showed interlacing bundles of spindle cells with eosihophilic cytoplasm and large vesicular nuclei(H&E, ×100). (B) The tumor cells show negative immunoreactivity for progesterone receptor on the nucleus(immunohistochemical stain,×200).
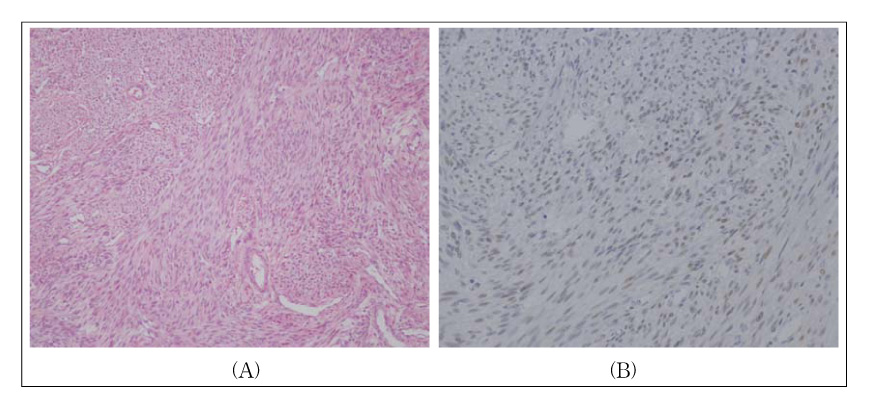
Figure 5 (A) The uterine mass showed higher celluar smooth muscle cells with multiply fascicular arragement(H&E,×100). (B) The tumor cells show positive immunoreactivity for progesterone receptor on the nucleus(immunohistochemical stain, ×200).
Reference
-
1. White SH, Ibrahim NB, Forrester-Wood CP, Jeyasingham K. Leiomyomas of the lower respiratory tract. Thorax. 1985. 40:306–311.2. Yellin A, Rosenman Y, Lieberman Y. Review of smooth muscle tumours of the lower respiratory tract. Br J Dis Chest. 1984. 78:337–351.3. Kayser K, Zink S, Schneider T, Dienemann H, Andre S, Kaltner H, et al. Benign metastasizing leiomyoma of the uterus: documentation of clinical, immunohistochemical and lectin-histochemical data of ten cases. Virchows Arch. 2000. 437:284–292.4. Steiner PE. Metastasizing fibroleiomyoma of the uterus: report of a case and review of the literature. Am J Pathol. 1939. 15:89–109.5. Arrigoni MG, Woolner LB, Bernatz PE, Miller WE, Fontana RS. Benign tumors of the lung: a ten-year surgical experience. J Thorac Cardiovasc Surg. 1970. 60:589–599.6. Ayabe H, Tsuji H, Tagawa Y, Tomita M, Tsuda N, Chen J. Endobronchial Leiomyoma: report of a case treated by bronchoplasty and a review of the literature. Surg Today. 1995. 25:1057–1060.7. Foroughi E. Leiomyoma of the trachea. Dis Chest. 1962. 42:230–232.8. Orlowski TM, Stasiak K, Kolodziej J. Leiomyoma of the lung. J Thorac Cardiovasc Surg. 1978. 76:257–261.9. Lee SC, Park MS, Chung JH, Kim YS, Kim KD, Chang J, et al. Two cases of bronchial leiomyoma initially misdiagnosed as bronchial asthma. Tuberc Respir Dis. 2003. 55:616–622.10. Yamada H, Katoh O, Yamaguchi T, Natsuaki M, Itoh T. Intrabronchial leiomyoma treated by localized resection via bronchotomy and bronchoplasty. Chest. 1987. 91:283–285.11. Choi JC, Yu CM, Ryu YJ, Jeon K, Choi KA, Kwon OJ, et al. The role of endoscopic surgery for completely obstructive endobronchial benign tumor. Korean J Intern Med. 2006. 21:15–19.12. Park SY, Lim EJ, Jang JS, Kim CH, Jee HK, Cho SJ, et al. Benign metastasizing pulmonary leiomyoma with hemoptysis. Tuberc Respir Dis. 2006. 60:92–96.13. Esteban JM, Allen WM, Schaerf RH. Benign metastasizing leiomyoma of the uterus: histologic and immunohistochemical characterization of primary and metastatic lesions. Arch Pathol Lab Med. 1999. 123:960–962.14. Banner AS, Carrington CB, Emory WB, Kittle F, Leonard G, Ringus J, et al. Efficacy of oophorectomy in lymphangioleiomyomatosis and benign metastasizing leiomyoma. N Engl J Med. 1981. 305:204–209.15. Hague WM, Abdulwahid NA, Jacobs HS, Craft I. Use of LHRH analogue to obtain reversible castration in a patient with benign metastasizing leiomyoma. Br J Obstet Gynaecol. 1986. 93:455–460.
