Superficial Esophageal Neoplasms Overlying Leiomyomas Removed by Endoscopic Submucosal Dissection: Case Reports and Review of the Literature
- Affiliations
-
- 1Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 2Department of Gastroenterology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. dohoon.md@gmail.com
- KMID: 1964276
- DOI: http://doi.org/10.5946/ce.2015.48.4.322
Abstract
- The coexistence of an epithelial lesion and a subepithelial lesion is uncommon. In almost all such cases, the coexistence of these lesions appears to be incidental. It is also extremely rare to encounter a neoplasm in the surface epithelium that overlies a benign mesenchymal tumor in the esophagus. Several cases of a coexisting esophageal neoplasm overlying a leiomyoma that is treated endoscopically or surgically have been reported previously. Here, three cases of a superficial esophageal neoplasm that developed over an esophageal leiomyoma and was then successfully removed by endoscopic submucosal dissection are described.
Figure
-
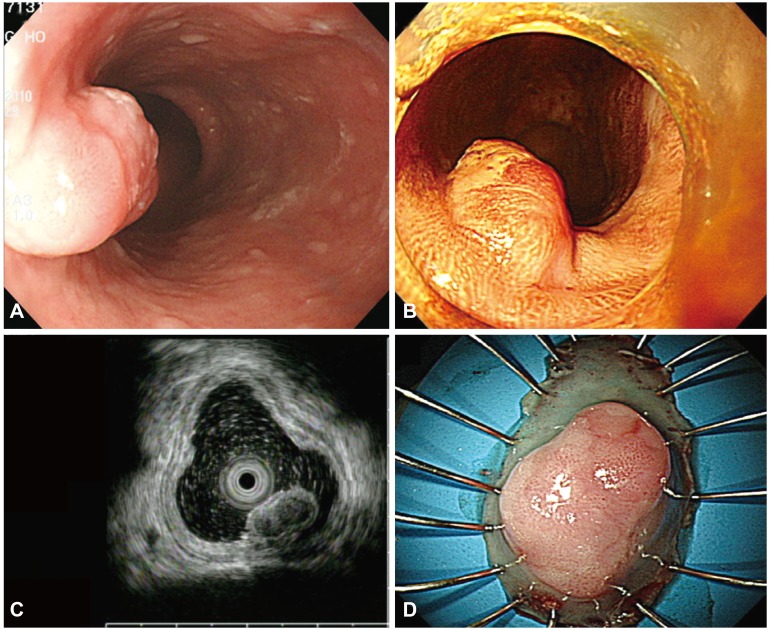
Fig. 1 (A) An endoscopic image shows a subepithelial tumor with an eroded surface in the middle third of the esophagus. (B) Lugol chromoendoscopy shows the iodine-unstained lesion. (C) Endoscopic ultrasonography demonstrates a hypoechoic, homogeneous lesion that originates from the muscularis mucosa and is covered by a squamous cell carcinoma in situ. (D) The specimen with the lesion after its en bloc resection.
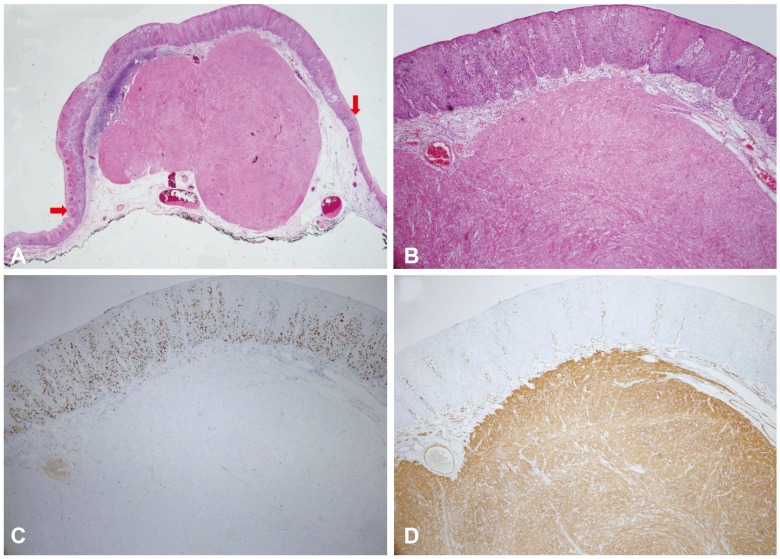
Fig. 2 (A) Histopathologically, the resected lesion is a squamous cell carcinoma that overlies a leiomyoma in situ. The red arrows correspond to the lateral margins of the squamous cell carcinoma (H&E stain, ×12.5). (B) The esophageal leiomyoma is composed of bland spindle cells with no mitosis or nuclear atypia (H&E stain, ×40). (C) The entire layer of atypical epithelial cells is positive for the Ki-67 stain and demonstrates a Ki-67 labeling index of less than 1% (×40). (D) The esophageal leiomyoma is strongly and diffusely positive for smooth muscle actin (×40).
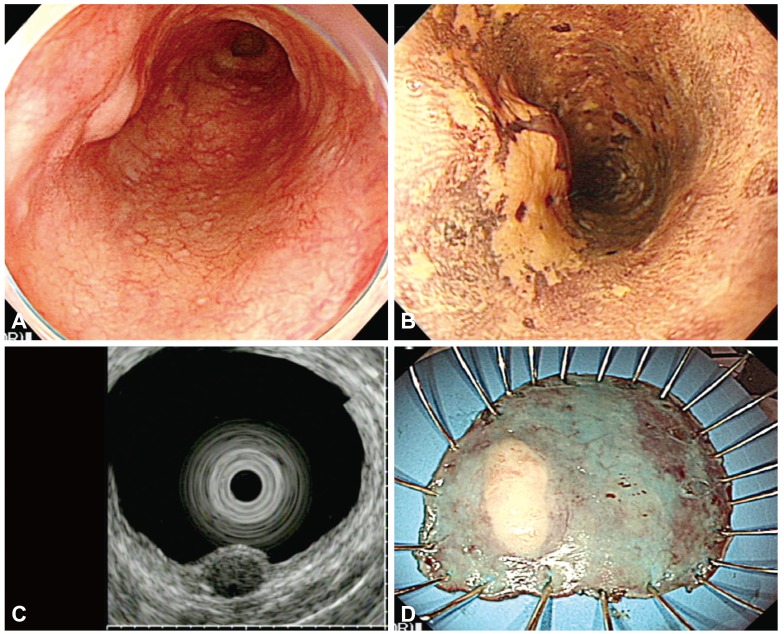
Fig. 3 (A) Endoscopic examination shows a subepithelial tumor with a flat hyperemic lesion in the upper esophagus. (B) Lugol chromoendoscopy shows the iodine-unstained lesion. (C) Endoscopic ultrasonography demonstrates a hypoechoic, homogeneous lesion that originates from the muscularis mucosa and is covered by a superficial squamous cell carcinoma. (D) The specimen with the lesion after en bloc resection.
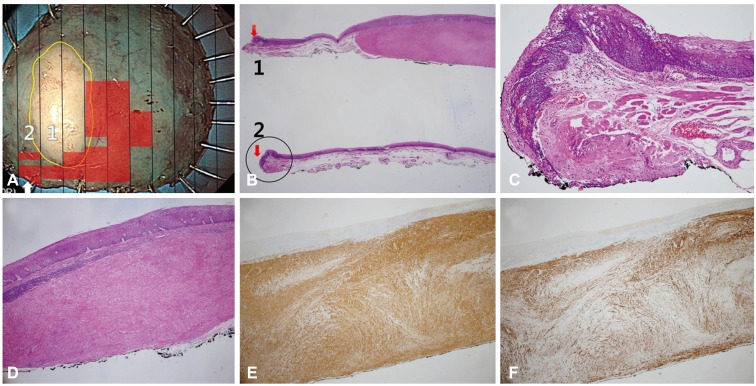
Fig. 4 (A) Histological mapping of the resected specimen shows severe dysplasia with a leiomyoma. The black lines indicate the cutting line of the block sections. The yellow circle corresponds to the leiomyoma and the red squares correspond to atypical squamous cells. The lateral margin is positive in section 2 (arrow). (B) There are two sections: section 1 is composed of leiomyoma and severe squamous cell dysplasia on the lateral portion (red arrow), and section 2 shows the positive lateral margin (H&E stain, ×12.5). (C) The positive margin can be seen when the black circle in Fig. 5B is magnified (H&E stain, ×100). (D) The specimen with the lesion is histologically diagnosed after resection as high-grade intraepithelial squamous neoplasia (H&E stain, ×40). (E) The esophageal leiomyoma is strongly and diffusely positive for smooth muscle actin (×40). (F) The esophageal leiomyoma is positive for desmin (×40).
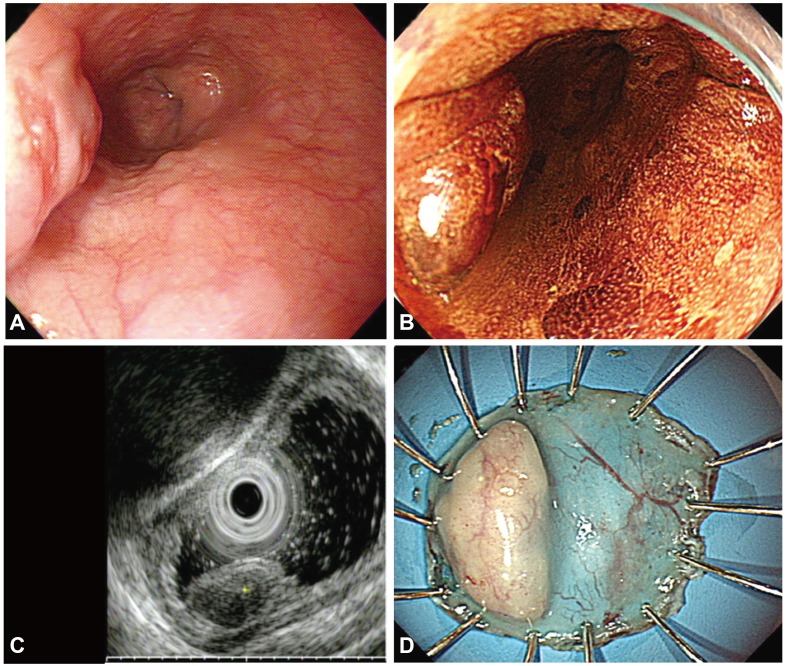
Fig. 5 (A) The endoscopic images show a subepithelial tumor with an eroded hyperemic lesion in the lower esophagus. (B) Lugol chromoendoscopy shows the iodine-unstained lesion. (C) Endoscopic ultrasonography demonstrates a hypoechoic, homogeneous lesion that originates from the muscularis mucosa and is covered by high-grade dysplasia. (D) The specimen with the lesion after en bloc resection.
Reference
-
1. Punpale A, Rangole A, Bhambhani N, et al. Leiomyoma of esophagus. Ann Thorac Cardiovasc Surg. 2007; 13:78–81. PMID: 17505413.2. Fountain SW. Leiomyoma of the esophagus. Thorac Cardiovasc Surg. 1986; 34:194–195. PMID: 2426836.
Article3. Postlethwait RW, Musser AW. Changes in the esophagus in 1,000 autopsy specimens. J Thorac Cardiovasc Surg. 1974; 68:953–956. PMID: 4420581.
Article4. Mutrie CJ, Donahue DM, Wain JC, et al. Esophageal leiomyoma: a 40-year experience. Ann Thorac Surg. 2005; 79:1122–1125. PMID: 15797036.
Article5. Iwaya T, Maesawa C, Uesugi N, et al. Coexistence of esophageal superficial carcinoma and multiple leiomyomas: a case report. World J Gastroenterol. 2006; 12:4588–4592. PMID: 16874880.
Article6. Iizuka T, Kato H, Watanabe H, Itabashi M, Hirota T. Superficial carcinoma of the esophagus coexisting with esophageal leiomyoma: a case report and review of the Japanese literature. Jpn J Clin Oncol. 1984; 14:115–122. PMID: 6708309.7. Mizobuchi S, Kuge K, Matsumoto Y, et al. Co-existence of early esophageal carcinoma and leiomyoma: a case report. Jpn J Clin Oncol. 2004; 34:751–754. PMID: 15640507.
Article8. Suzuki H, Nagayo T. Primary tumors of the esophagus other than squamous cell carcinoma: histologic classification and statistics in the surgical and autopsied materials in Japan. Int Adv Surg Oncol. 1980; 3:73–109. PMID: 6926744.9. Ahn SY, Jeon SW. Endoscopic resection of co-existing severe dysplasia and a small esophageal leiomyoma. World J Gastroenterol. 2013; 19:137–140. PMID: 23326177.
Article10. Ishida M, Mochizuki Y, Iwai M, Yoshida K, Kagotani A, Okabe H. Esophageal squamous cell carcinoma in situ overlying leiomyoma: a case report with review of the literature. Int J Clin Exp Pathol. 2013; 6:3026–3028. PMID: 24294396.11. Niimi K, Kodashima S, Ono S, Goto O, Yamamichi N, Fujishiro M. Curative ESD for intraepithelial esophageal carcinoma with leiomyoma mimicking submucosal invasive carcinoma. World J Gastrointest Endosc. 2009; 1:68–71. PMID: 21160655.
Article12. Ishihara R, Yamamoto S, Yamamoto S, et al. Endoscopic resection of the esophageal squamous cell carcinoma overlying leiomyoma. Gastrointest Endosc. 2008; 67:745–747. PMID: 18206883.
Article13. Joo SY, Lee WS, Park SY, et al. A case of esophageal carcinoma coexisting with leiomyoma removed by endoscopic resection. Korean J Gastrointest Endosc. 2007; 34:324–328.14. Fu KI, Muto M, Mera K, et al. Carcinoma coexisting with esophageal leiomyoma. Gastrointest Endosc. 2002; 56:272–273. PMID: 12145610.
Article15. Nagashima R, Takeda H, Motoyama T, Tsukamoto O, Takahashi T. Coexistence of superficial esophageal carcinoma and leiomyoma: case report of an endoscopic resection. Endoscopy. 1997; 29:683–684. PMID: 9360884.
Article16. Kuwano H, Sadanaga N, Watanabe M, Yasuda M, Nozoe T, Sugimachi K. Esophageal squamous cell carcinoma occurring in the surface epithelium over a benign tumor. J Surg Oncol. 1995; 59:268–272. PMID: 7630176.
Article17. Sarbia M, Katoh E, Borchard F. Collision tumor of squamous cell carcinoma and leiomyoma in the esophagus. Pathol Res Pract. 1993; 189:360–362. PMID: 8332578.
Article18. Ono S, Fujishiro M, Koike K. Endoscopic submucosal dissection for superficial esophageal neoplasms. World J Gastrointest Endosc. 2012; 4:162–166. PMID: 22624067.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Treatment for Esophageal Cancer
- Endoscopic Resection for the Treatment of Superficial Esophageal Neoplasms
- Pyloric Gland Adenoma of the Esophagus Treated by Endoscopic Submucosal Dissection: A Case Report
- Intralesional Steroid Injection to Prevent Stricture after Near-Circumferential Endosopic Submucosal Dissection for Superficial Esophageal Cancer
- Endoscopic Submucosal Dissection for Recurrent or Residual Superficial Esophageal Cancer after Chemoradiotherapy: Two Cases
