Ruptured Tricuspid Valve Papillary Muscle in a Neonate with Intractable Persistent Fetal Circulation
- Affiliations
-
- 1Department of Pediatrics, Seoul National University Children's Hospital, Seoul, Korea. eunjbaek@snu.ac.kr
- 2Department of Thoracic & Cardiovascular Surgery, Seoul National University Children's Hospital, Seoul, Korea.
- KMID: 1964108
- DOI: http://doi.org/10.4070/kcj.2015.45.4.340
Abstract
- Unguarded tricuspid regurgitation (TR) due to a flail tricuspid leaflet is a rare condition of newborn cyanosis. A high perinatal mortality has been associated with this fatal condition. But, there are feasible surgical repairs to improve survival. We report the case of a male full-term neonate with intractable hypoxia. He had profound tricuspid insufficiency and leaflet prolapse caused by a ruptured papillary muscle supporting the anterior leaflet of the tricuspid valve. He presented with severe cyanosis and respiratory distress immediately after birth. Despite medical management, the pulmonary vascular resistance was not decreased and a low cardiac output persisted. Initial stabilization was accomplished with nitric oxide and extracorporeal membrane oxygenation. The tricuspid valve repair surgery was successfully performed subsequently. TR resulting from papillary muscle rupture is a potentially lethal condition. Timely diagnosis and proper surgical treatment can be lifesaving.
MeSH Terms
-
Anoxia
Cardiac Output, Low
Cyanosis
Diagnosis
Extracorporeal Membrane Oxygenation
Female
Humans
Infant, Newborn*
Male
Nitric Oxide
Papillary Muscles*
Parturition
Perinatal Mortality
Persistent Fetal Circulation Syndrome*
Prolapse
Rupture
Thoracic Surgery
Tricuspid Valve Insufficiency
Tricuspid Valve*
Vascular Resistance
Nitric Oxide
Figure
-

Fig. 1 Anterior-posterior chest radiograph. A: on admission, a right pneumothorax with mediastinal shifting is observed. B: after chest tube insertion for the pneumothorax, cardiomegaly is not severe. C: thirty hours after birth, cardiomegaly has not progressed; however, the pulmonary vascular marking has decreased.
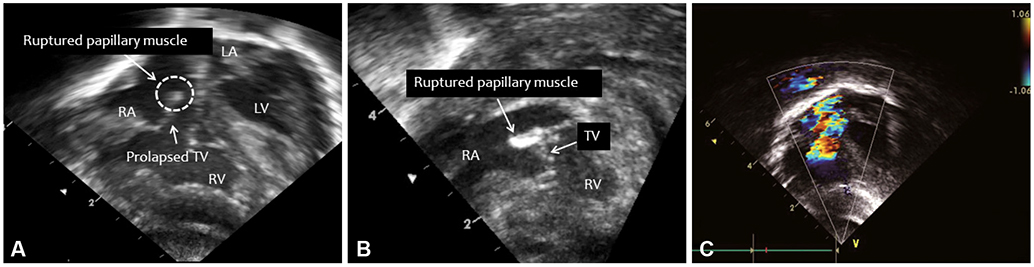
Fig. 2 Apical four chamber echocardiographic image shows a flail anterior leaflet of the tricuspid valve. The thick end (arrow, A) of the leaflet is the ruptured papillary muscle, which is documented more clearly with cine imaging (B), and the severe tricuspid regurgitation is documented by color Doppler imaging (C). LA: left atrium, LV: left ventricle, RA: right atrium, RV: right ventricle, TV: tricuspid valve.
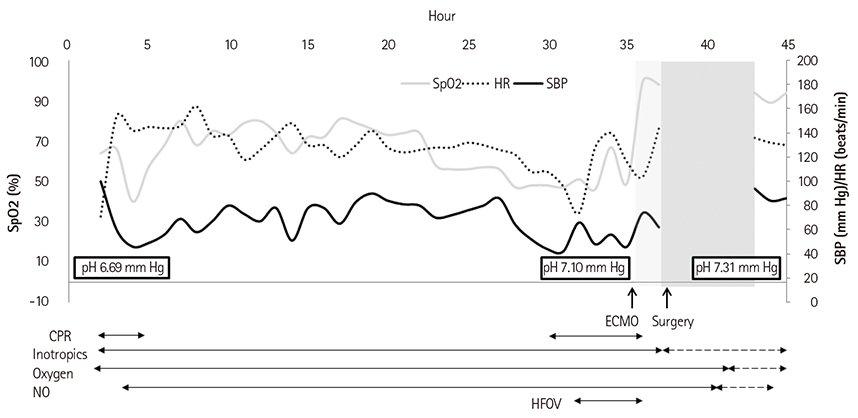
Fig. 3 The neonate shows intractable hypoxemia and cardiac shock despite treatment. After ECMO support and surgery, the vital signs stabilize, and the demand of inotropic drugs, NO, and oxygen is decreased. SpO2: saturation by pulse oximetry, HR: heart rate, SBP: systolic blood pressure, CPR: cardiopulmonary resuscitation, HFOV: high frequency oscillatory ventilator, ECMO: extracorporeal membrane oxygenation.
Reference
-
1. Alkalay AL, Ferry DA, Pepkowitz SH, Chou PJ, Oakes GK, Pomerance JJ. Critical tricuspid insufficiency due to papillary muscle rupture. A result of prenatal hypoxic insult. Am J Dis Child. 1988; 142:753–755.2. Sachdeva R, Fiser RT, Morrow WR, Cava JR, Ghanayem NS, Jaquiss RD. Ruptured tricuspid valve papillary muscle: a treatable cause of neonatal cyanosis. Ann Thorac Surg. 2007; 83:680–682.3. Lim KA, Huh J, Jun TG. Successful repair of critical tricuspid regurgitation secondary to ruptured papillary muscle in a newborn. Cardiol Young. 2004; 14:450–452.4. Arrington CB, Kouretas PC, Mart CR. Extracorporeal membrane oxygenation as a bridge to surgical treatment of flail tricuspid valve in a neonate. Cardiol Young. 2005; 15:660–662.5. De Busk RF, Harrison DC. The clinical spectrum of papillary-muscle disease. N Engl J Med. 1969; 281:1458–1467.6. Benvenuti LA, Aiello VD, Cury AJ, Ebaid M. Post-ischemic rupture of the anterior papillary muscle of the right ventricle associated with persistent pulmonary hypertension of the newborn: a case report. Am J Cardiovasc Pathol. 1992; 4:79–84.7. Fleming GA, Scholl FG, Kavanaugh-McHugh A, Liske MR. A case of an infant with flail tricuspid valve due to spontaneous papillary muscle rupture: was neonatal lupus the culprit? Pediatr Cardiol. 2008; 29:442–445.8. Yemul MA. A flail anterior tricuspid leaflet secondary to anteroposterior papillary muscle rupture in a neonate. Echocardiography. 2014; 31:E151–E155.9. Anagnostopoulos PV, Alphonso N, Nölke L, et al. Neonatal mitral and tricuspid valve repair for in utero papillary muscle rupture. Ann Thorac Surg. 2007; 83:1458–1462.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Successful Repair of Critical Tricuspid Regurgitation Secondary to a Ruptured Papillary Muscle in a Neonate
- Repair of Ruptured Papillary Muscle of the Tricuspid Valve as a Cause of Tricuspid Insufficiency Following Blunt Chest Trauma
- Post-traumatic tricuspid regurgitation with anterior papillary muscle rupture, corrected by papillary muscle reimplantation
- The Morphologic Study of the Tricuspid Valve Complex in Korean Adult Hearts
- Simultaneous Aortic and Tricuspid Valve Endocarditis due to Complication of Sinus of Valsalva Rupture
