Familial tooth bone graft for ridge and sinus augmentation: a report of two cases
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, Section of Dentistry, Seoul National University Bundang Hospital, Seongnam, Korea.
- 2Department of Oral and Maxillofacial Surgery, School of Dentistry, Chosun University, Gwangju, Korea. sgckim@chosun.ac.kr
- 3Department of Pathology, School of Medicine, Chosun University, Gwangju, Korea.
- KMID: 1960971
- DOI: http://doi.org/10.5125/jkaoms.2014.40.1.37
Abstract
- Recently, clinical application of autogenous tooth bone-graft materials has been reported. Autogenous tooth bone graft has been used in implant surgery. Familial tooth bone graft is a more advanced procedure than autogenous teeth bone graft in that extracted teeth can be used for bone graft materials of implant and teeth donation between siblings is possible. We used autogenous tooth and familial tooth bone-graft materials for ridge augmentation and sinus bone graft and obtained satisfactory results. The cases are presented herein.
Figure
-

Fig. 1 A photograph of the oral cavity prior to surgery.

Fig. 2 A panorama radiograph at the initial diagnosis. The dentist at another clinic was expected to place implants in the #13 and #23 areas. The patient was referred to us for horizontal augmentation. The #48 area was planned for extraction and used as bone graft material.

Fig. 3 A panorama radiograph of a 15-year-old female patient who was the daughter of the patient. The decision was made to extract the #18 and #48 impacted molars and prepare them as block and powder bone-graft materials.
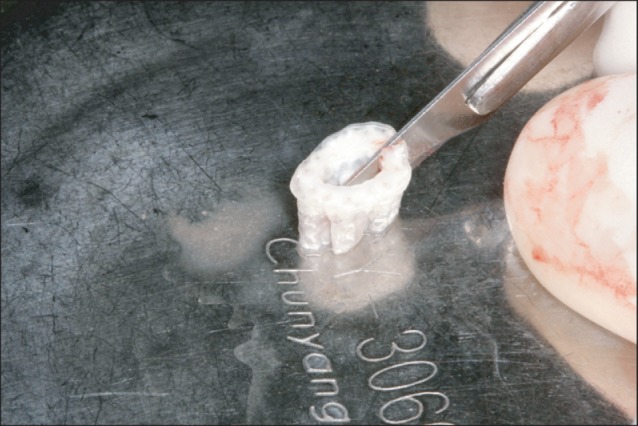
Fig. 4 The appearance of trimmed familial tooth bone blocks. Block-type graft materials were hydrated for 30 minutes in normal saline, divided to two blocks with a #15 blade.
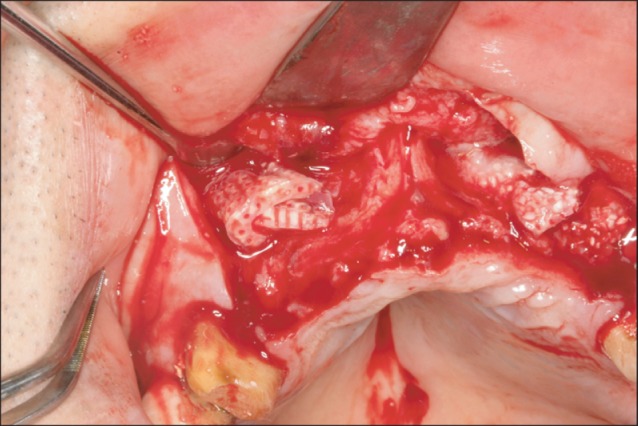
Fig. 5 Insertion of the block to the labial side of the maxillary canine area. It was not specially fixed with screws.
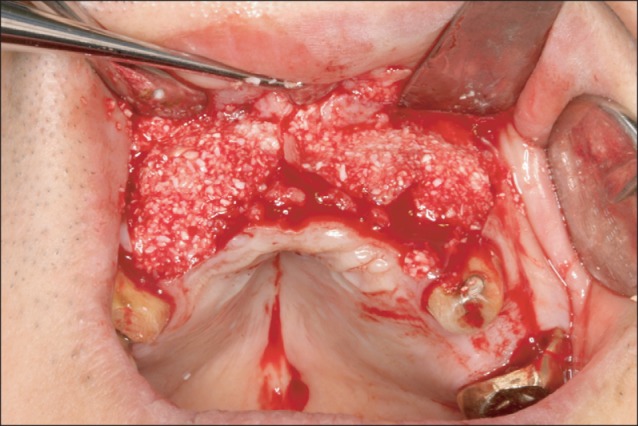
Fig. 6 The appearance after grafting powder-type bone-graft materials in the vicinity of the block.
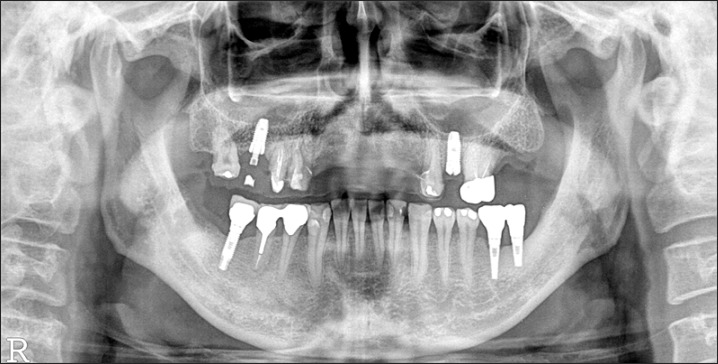
Fig. 7 A panorama radiograph taken 5 months after bone graft. During the healing period, implants were placed in the maxillary left 2nd premolar area in a local clinic.

Fig. 8 The appearance after implant placement. Eight months after bone graft, in a local clinic, 4 implants were placed in a non-submerged type. The early fixation was excellent, and thus, after 1 week, a temporary prosthesis was installed (Anyang More Dental Clinic, Byoengdoek Yu and Gyuhyong Lee's case).

Fig. 9 A panoramic radiograph taken 3 months after the installation of a temporary prosthesis (Anyang More Dental Clinic, Byoengdoek Yu and Gyuhyong Lee's case).

Fig. 10 A panorama radiograph at the time of initial diagnosis. The abscess in the #25 root apex and periodontitis in the #15-#16 were in severe condition. The decision was made to first treat the left maxillary molar area. We planned to extract the #48 and treat with autogenous tooth bone-graft materials.

Fig. 11 A panorama radiograph of the 22-year-old son. The #28 and #38 teeth were extracted and prepared as powder bone-graft materials.
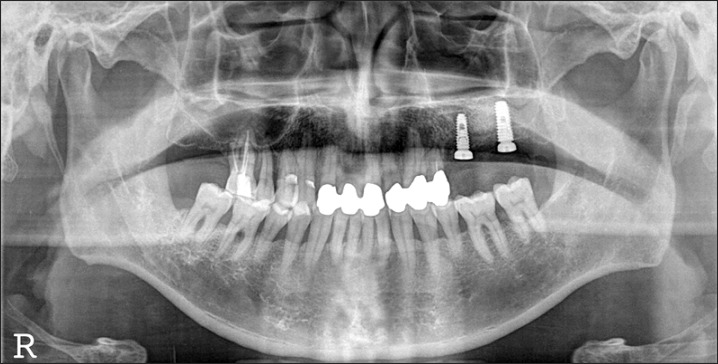
Fig. 12 A panorama radiograph after implant placement. Implants were placed 3 months after bone graft.
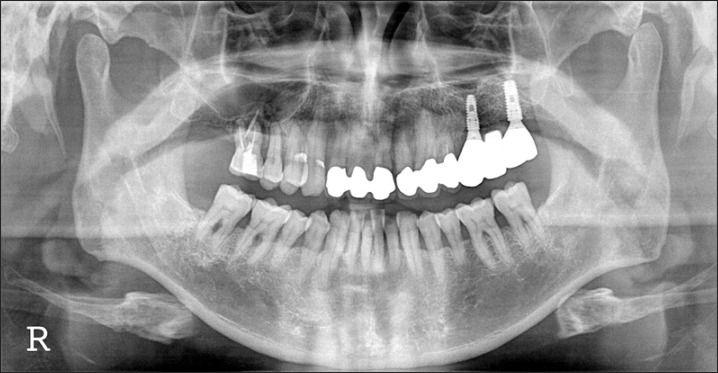
Fig. 13 A panorama radiograph 24 months after final prosthetic delivery.
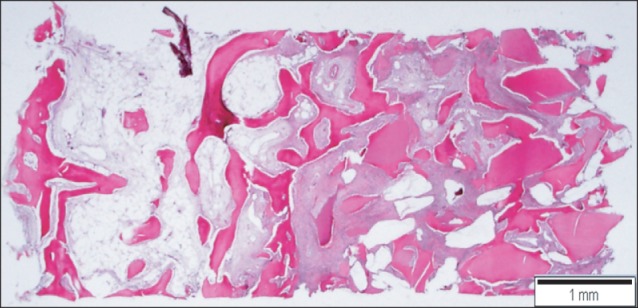
Fig. 14 Scanning view of the implantation site. New bone formation is demonstrated around the implant materials. Left: residual alveolar bone site, right: sinus bone graft area. H&E staining, scale bar=1 mm.
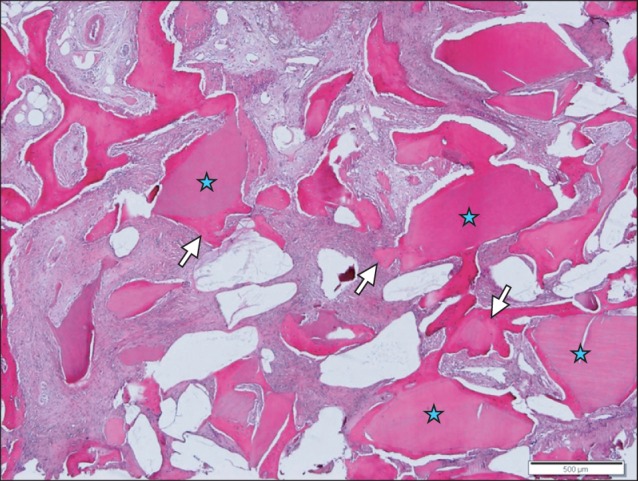
Fig. 15 New bone forming anastomosing trabeculae (arrows) is identified around the implant materials (asterisks). H&E staining, scale bar=500 µm.
Reference
-
1. Kim YK, Yi YJ, Yun PY, Yeo IS, Lee HJ, Kim SG, et al. All about implants in Q&A (I). Yongin: Korea Quintessence;2010. p. 304–331.2. Kim SG, Lee BG. Bone graft and implant. Vol. 2-2. Clinical application of a variety of bone graft. Seoul: Narae Publishing;2007. p. 240–258.3. Del Fabbro M, Testori T, Francetti L, Weinstein R. Systematic review of survival rates for implants placed in the grafted maxillary sinus. Int J Periodontics Restorative Dent. 2004; 24:565–577. PMID: 15626319.
Article4. Kim YK, Kim SG, Byeon JH, Lee HJ, Um IU, Lim SC, et al. Development of a novel bone grafting material using autogenous teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010; 109:496–503. PMID: 20060336.
Article5. Kim SJ, Kim YM, Kim MR. Present and future of autogenout tooth graft. Dent Success. 2010; 30:790–800.6. Korea Auto-Tooth and Bone Bank Committee. Familial tooth bank standards. 2010.7. Pearson KA, Brubaker SA, Anderson ML. Standards for tissue banking. 12th ed. McLean: American Association of Tissue Banks (AATB);2008. p. 13–108.8. Barrett AP, Reade PC. A histological investigations of isografts of immature mouse molars to an intrabony and extrabony site. Arch Oral Biol. 1982; 27:59–63. PMID: 6951529.9. Barrett AP, Reade PC. A histological investigation of isografts of mature mouse molars to an intrabony and an extrabony site. Transplantation. 1981; 31:353–357. PMID: 7233533.10. Steidler NE, Reade PC. An histological study of the effects of extra-corporeal time on murine dental isografts. Arch Oral Biol. 1979; 24:165–169. PMID: 299142.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ridge Augmentation Using Block Type of Autogenous Tooth Bone Graft Material in Severe Alveolar Bone Resorption of Single Tooth: Case Report
- SINUS GRAFT AND VERTICAL AUGMENTATION OF MAXILLARY POSTERIOR ALVEOLAR RIDGE USING MANDIBULAR RAMAL BLOCK BONE GRAFT
- Vertical and Horizontal Ridge Augmentation Using Autogenous Tooth Bone Graft Materials: Case Report
- Vertical Augmentation of Maxillary Posterior Alveolar Ridge Using Allogenic Block Bone Graft and Simultaneous Maxillary Sinus Graft
- Combined Sinus Floor and Alveolar Ridge Augmentation Simultaneously Performed with Extraction of Ankylosed Maxillary Molar: A Case Report
