Brain Neurorehabil.
2014 Mar;7(1):48-53. 10.12786/bn.2014.7.1.48.
Functional Outcomes of Patients with Severe MCA Infarction after Decompressive Craniectomy
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, Dong-A University College of Medicine, Korea. jun7432@hotmail.com
- KMID: 1914559
- DOI: http://doi.org/10.12786/bn.2014.7.1.48
Abstract
OBJECTIVE
To compare the functional outcomes between surgical treatment and conservative medical treatment for severe middle cerebral artery (MCA) infarction. METHOD: This is comparative analysis of prospectively documented data with 25 patients have malignant MCA infarction. Ten patients in Group A (male 7, female 3) received surgical treatment such as decompressive craniectomy, and fifteen patients in Group B (male 10, female 5) received conservative medical treatment. We defined MCA infarction as "severe" when it concerned both the deep and superficial areas of the MCA or when the Functional Independence Measure (FIM) was lower to 75 on admission to our department. Functional status was measured using modified Rankin Scale (mRS), FIM, Motricity Index (MI) and Trunk Control Test (TCT). All evaluations were measured at baseline and 90 days after stroke.
RESULTS
Mean age were 55.0 +/- 8.6 and 58.7 +/- 12.3 in Group A and B. Rt. MCA infarction were 4 in Group A and 5 in Group B. Lt. MCA infarction were 5 in Group A and 10 in Group B. Baseline functional status between two groups was not significantly different. Each group showed functional improvement according to the time. When compared changes between two groups, arm Motricity Index, K-MMSE, mRS and FIM were no significant difference between two groups. Leg segments of MI and TCT was significantly improved in Group A more than B at 90 days after baseline evaluation (p<0.05).
CONCLUSION
Decompressive craniectomy improved motor function of affected leg and trunk in patients with severe MCA infarction more than conservative medical treatment alone.
MeSH Terms
Figure
-
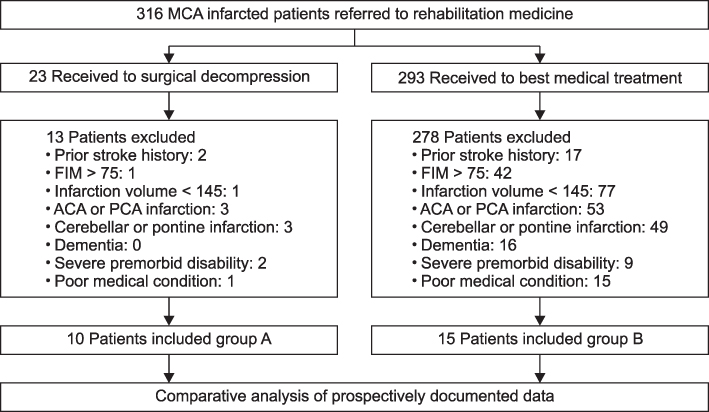
Fig. 1 Flow chart of patient group assignment and treatment.
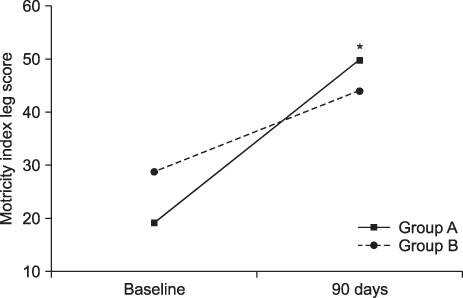
Fig. 2 Change of Trunk Control Test in both groups. Group A: Patients with decompressive craniectomy. Group B: Patients without decompressive craniectomy. *p<0.05.
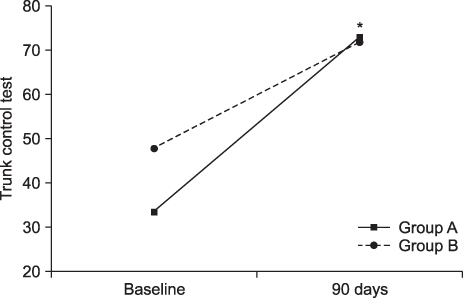
Fig. 3 Change of Motricity Index leg score in both groups. Group A: Patients with decompressive craniectomy. Group B: Patients without decompressive craniectomy. *p<0.05.
Reference
-
1. Heinsius T, Bogousslavsky J, Van Melle G. Large infarcts in the middle cerebral artery territory: etiology and outcome patterns. Neurology. 1998; 50:341–350.2. Mandon L, Bradaï N, Guettard E, Bonan I, Vahedi K, Bousser MG, Yelnik A. Do patients have any special medical or rehabilitation difficulties after a craniectomy for malignant cerebral infarction during their hospitalization in a physical medicine and rehabilitation department? Ann Phys Rehabil Med. 2010; 53:86–95.3. Hacke W, Schwab S, Horn M, Spranger M, De Georgia M, von Kummer R. Malignant middle cerebral artery territory infarction: clinical course and prognostic signs. Arch Neurol. 1996; 53:309–315.4. Bereczki D, Liu M, do Parado GF, Fekete I. Mannitol for acute stroke. Stroke. 2008; 39:512–513.5. Righetti E, Celani MG, Cantisani T, Sterzi R, Boysen G, Ricci S. Glycerol for acute stroke. J Neurol. 2002; 249:445–451.6. Hofmeijer J, van der Worp HB, Kappelle LJ. Treatment of spaceoccupying cerebral infarction. Crit Care Med. 2003; 31:617–625.7. Schwarz S, Schwab S, Bertram M, Aschoff A, Hacke W. Effects of hypertonic saline hydroxyethyl starch solution and mannitol in patients with increased intracranial pressure after stroke. Stroke. 1998; 29:1550–1555.8. Schwarz S, Georgiadis D, Aschoff A, Schwab S. Effects of body position on intracranial pressure and cerebral perfusion in patients with large hemispheric stroke. Stroke. 2002; 33:497–501.9. Schwab S, Spranger M, Schwarz S, Hacke W. Barbiturate coma in severe hemispheric stroke: useful or obsolete? Neurology. 1997; 48:1608–1613.10. Schwab S, Steiner T, Aschoff A, Schwartz S, Steiner HH, Jansen O, Hacke W. Early hemicraniectomy in patients with complete middle cerebral infarction. Stroke. 1998; 29:1888–1893.11. Vahedi K, Hofmeijer J, Juettler E, Vicaut E, George B, Algra A, Amelink GJ, Schmiedeck P, Schwab S, Rothwell PM, Bousser MG, van der Worp HB, Hacke W. Early decompressive surgery in malignant middle cerebral artery infarction: a pooled analysis of three randomised controlled trials. Lancet Neurol. 2007; 6:215–222.12. Vahedi K, Vicaut E, Mateo J, Kurtz A, Orabi M, Guichard JP, Boutron C, Couvreur G, Rouanet F, Touzé E, Guillon B, Carpentier A, Yelnik A, George B, Payen D, Bousser MG. DECIMAL Investigators. Sequential-design, multicenter, randomized, controlled trial of early decompressive craniectomy in malignant middle cerebral artery infarction (DECIMAL Trial). Stroke. 2007; 38:2506–2517.13. Walz B, Zimmermann C, Bottger S, Haberl RL. Prognosis of patients after hemicraniectomy in malignant middle cerebral artery infarction. J Neurol. 2002; 249:1183–1190.14. Hofmeijer J, Kappelle LJ, Algra A, Amelink GJ, van Gijn J, van der Worp HB. Surgical decompression for space-occupying cerebral infarction (the Hemicraniectomy After Middle Cerebral Artery infarction with Life-threatening Edema Trial [HAMLET]): a multicentre, open, randomised trial. Lancet Neurol. 2009; 8:326–333.15. Gialanella B, Bertolinelli M, Santoro R. Rehabilitative outcome in supratentorial and infratentorial stroke: The role of motor deficits. Aging Clin Exp Res. 2008; 20:310–315.16. Walz B, Zimmermann C, Bottger S, Haberl RL. Prognosis of patients after hemicraniectomy in malignant middle cerebral artery infarction. J Neurol. 2002; 249:1183–1190.17. Jüttler E, Schwab S, Schmiedek P, Unterberg A, Hennerici M, Woitzik J, Witte S, Jenetzky E, Hacke W. DESTINY Study Group. Decompressive Surgery for the Treatment of Malignant Infarction of the Middle Cerebral Artery (DESTINY): a randomized, controlled trial. Stroke. 2007; 38:2518–2525.18. Doerfler A, Forsting M, Reith W, Staff C, Heiland S, Schäbitz WR, von Kummer R, Hacke W, Sartor K. Decompressive craniectomy in a rat model of "malignant" cerebral hemispherical stroke: experimental support for an aggressive therapeutic approach. J Neurosurg. 1996; 85:853–859.19. Forsting M, Reith W, Schäbitz WR, Heiland S, von Kummer R, Hacke W, Sartor K. Decompressive craniectomy for cerebral infarction: an experimental study in rats. Stroke. 1995; 26:259–264.20. Dujovny M, Aviles A, Agner C, Fernandez P, Charbel T. Cranioplasty: Cosmetic or therapeutic? Surg Neurol. 1997; 47:238–241.21. van der Worp HB, Kappelle LJ. Early decompressive hemicraniectomy in older patients with nondominant hemispheric infarction does not improve outcome. Stroke. 2011; 42:845–846.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Outcome Following Decompressive Craniectomy for Malignant Middle Cerebral Artery Infarction in Patients Older Than 70 Years Old
- The Effectiveness of Decompressive Craniectomy with Dural Augmentation in Malignant Cerebral Infarction
- Efficacy of the Decompressive Craniectomy for Acute Cerebral Infarction: Timing of Surgical Intervention and Clinical Prognostic Factors
- Clinical Comparison between Simple Craniectomy and Lesionectomy in the Patients with Acute Cerebral Infarction
- Therapeutic Hypothermia for Increased Intracranial Pressure after Decompressive Craniectomy: A Single Center Experience
