A Clinical Observation of Patients with Hypertrophic Cardiomyopathy and Implantable Cardioverter-Defibrillators
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. youho@amc.seoul.kr
- KMID: 1909619
- DOI: http://doi.org/10.4070/kcj.2007.37.11.574
Abstract
-
BACKGROUND AND OBJECTIVES: Hypertrophic cardiomyopathy (HCM) is one of the most common heritable cardiac diseases. Patients with HCM are prone to ventricular tachyarrhythmias, and implantable cardioverter-defibrillator (ICD) implantation is recommended in high-risk patients to prevent sudden death. Clinical and tachycardial characteristics in patients with HCM have not been studied systematically.
SUBJECTS AND METHODS
Between April 1996 and February 2006, 23 patients with HCM underwent implantation of ICDs. ICDs were indicated for primary prevention in 9 patients and for secondary prevention in 14 patients. Clinical features, follow-up events and intracardiac electrograms were reviewed.
RESULTS
During a median follow-up period of 561 days (range 16 to 2,694 days), a total of 51 episodes of ventricular tachycardia (VT) occurred in 6 patients, while only one episode of ventricular fibrillation (VF) was recorded. There were 45 (64.2%) appropriate shocks [30 defibrillation shocks in 5 patients and 15 antitachycardia pacings (ATP) in 2 patients] in 6 patients, and 25 (35.7%) inappropriate shocks in 7 patients. The coupling intervals and VT cycle lengths were highly variable within individual patients. Over-drive acceleration in response to ATP was observed in 1 patient.
CONCLUSION
As ventricular tachycardia is the main ventricular tachyarrhythmia in patients with HCM, an empirical ATP setting for VTs appears to be mandatory even in patients without previously documented VT. Based on the analyses of the intracardiac electrograms (presence of overdrive acceleration, variations in coupling intervals and cycle lengths), triggered activity may have an important role in the mechanism of a ventricular tachycardia.
Keyword
MeSH Terms
-
Acceleration
Adenosine Triphosphate
Cardiomyopathy, Hypertrophic*
Death, Sudden
Death, Sudden, Cardiac
Defibrillators, Implantable*
Electrophysiologic Techniques, Cardiac
Follow-Up Studies
Heart Diseases
Humans
Primary Prevention
Secondary Prevention
Shock
Tachycardia
Tachycardia, Ventricular
Ventricular Fibrillation
Adenosine Triphosphate
Figure
-
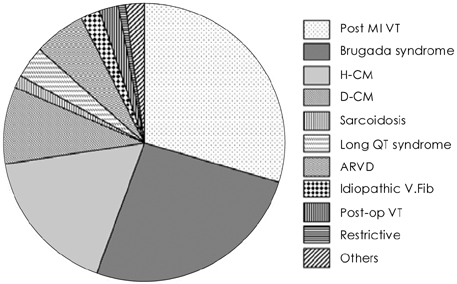
Fig. 1 The Indications for ICD implantation at Asan Medical Center. Post-MI VT, Brugada syndrome, HCM were the three major causes of ICD implantation at Asan Medical Center. In 17% of total ICD implantations, HCM was the underlying heart disease. MI: myocardial infarction, VT: ventricular tachycardia, HCM: hypertrophic cardiomyopathy, DCM: dilated cardiomyopathy, ARVD: arrhythmogenic right ventricular dysplasia, Post-op: post-operation.

Fig. 2 A marked variation in the coupling interval and ventricular tachycardial cycle length (Patient number 3). The panel A, B, C show 3 intracardiac electrograms recorded from patient number 3 during different VT events. The coupling intervals were 531, 875, 805 msec respectively (indicated as double-headed arrows), and the mean VT cycle lengths were 370, 336, 429 msec respectively for each episode. Within the same patient, coupling intervals and VT cycle lengths were highly variable. VT: ventricular tachycardia.
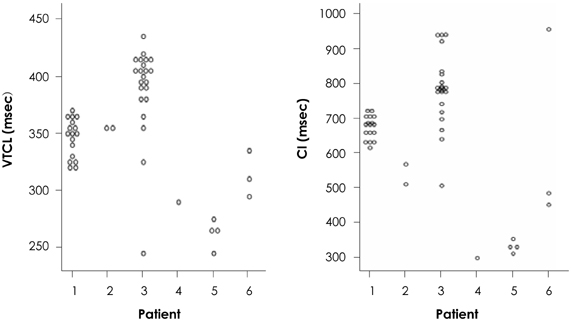
Fig. 3 Distribution of coupling intervals and ventricular tachycardial cycle lengths. Coupling intervals and VT cycle lengths were measured by analyzing intracardiac electrograms recorded on ICDs. Coupling intervals and VT cycle lengths were highly variable within each patient. VTCL: ventricular tachycardial cycle length, CI: coupling interval, VT: ventricular tachycardia, ICD: implantable cardioverter-defibrillator.
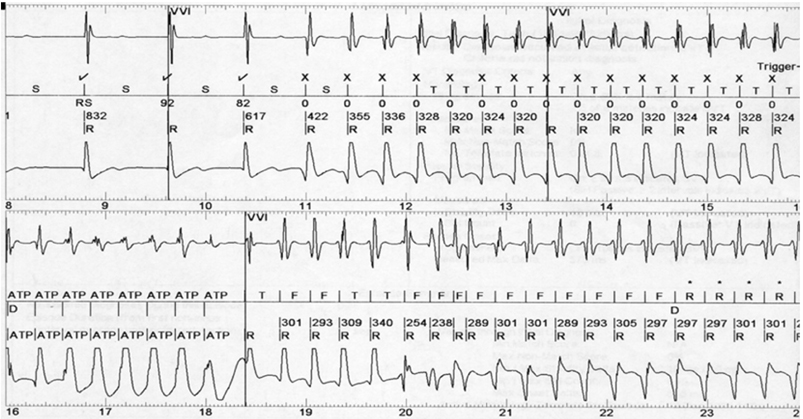
Fig. 4 An example of overdrive acceleration in patient number 1. An example of overdrive acceleration is shown. The VT cycle length is changed from an average of 333±27 msec to 294±22 msec after anti-tachycardia pacing. This was subsequently terminated by a defibrillation shock (not shown on the figure). VT: ventricular tachycardia.
Reference
-
1. Jeong JW. Hypertrophic cardiomyopathy. Korean Circ J. 2002. 32:7–14.2. Maron BJ, Shen WK, Link MS, et al. Efficacy of implantable cardioverter-defibrillators for the prevention of sudden death in patients with hypertrophic cardiomyopathy. N Engl J Med. 2000. 342:365–373.3. Kim DH, Kim SY, Lee KH, et al. Follow up of a group of patients with automatic implantable defibrillator. Korean Circ J. 2005. 35:69–83.4. Lee DI, Kim AS, Kim JY, et al. Implantable cardioverter-defibrillator (ICD) therapy: initial clinical experience in 6 patients. Korean Circ J. 1999. 29:999–1015.5. Kuck KH, Cappato R, Siebels J, Ruppel R. Randomized comparison of antiarrhythmic drug therapy with implantable defibrillators in patients resuscitated from cardiac arrest: the Cardiac Arrest Study Hamburg (CASH). Circulation. 2000. 102:748–754.6. Maron BJ, Estes NA 3rd, Maron MS, Almquist AK, Link MS, Udelson JE. Primary prevention of sudden death as a novel treatment strategy in hypertrophic cardiomyopathy. Circulation. 2003. 107:2872–2875.7. Jayatilleke I, Doolan A, Ingles J, et al. Long-term follow-up of implantable cardioverter defibrillator therapy for hypertrophic cardiomyopathy. Am J Cardiol. 2004. 93:1192–1194.8. Begley DA, Mohiddin SA, Tripodi D, Winkler JB, Fananapazir L. Efficacy of implantable cardioverter defibrillator therapy for primary and secondary prevention of sudden cardiac death in hypertrophic cardiomyopathy. Pacing Clin Electrophysiol. 2003. 26:1887–1896.9. Kim YH, Kim JS. Clinical characteristics in patients with implantable cardioverter-defibrillator (ICD). Korean Circ J. 2004. 34:395–404.10. Fananapazir L, Chang AC, Epstein SE, McAreavey D. Prognostic determinants in hypertrophic cardiomyopathy: prospective evaluation of a therapeutic strategy based on clinical, Holter, hemodynamic, and electrophysiological findings. Circulation. 1992. 86:730–740.11. Sweeney MO, Wathen MS, Volosin K, et al. Appropriate and inappropriate ventricular therapies, quality of life, and mortality among primary and secondary prevention implantable cardioverter defibrillator patients: results from the Pacing Fast VT REduces Shock ThErapies (PainFREE Rx II) trial. Circulation. 2005. 111:2898–2905.12. Josephson M. Clinical Cardiac Electrophysiology, Techniques and Interpretations. 2nd ed. Lea & Febiger;502–506.13. Behr ER, Elliott P, McKenna WJ. Role of invasive EP testing in the evaluation and management of hypertrophic cardiomyopathy. Card Electrophysiol Rev. 2002. 6:482–486.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Updated risk assessments for sudden cardiac death in hypertrophic cardiomyopathy patients with implantable cardioverter-defibrillator
- Implantable Cardioverter-defibrillator for Primary Prevention of Sudden Cardiac Death in Non-ischemic Cardiomyopathy
- A Case Report of the Patient Implanted with Automatic Implantable Cardioverter Defibrillator (AICD) Subject to 3rd Molar Extraction using Target Controlled Infusion of Propofol and Remifentanil: A Case Report
- Transvenous Implantation of an Implantable Cardioverter Defibrillator in a Patient Who Had Undergone Tricuspid Valve Replacement
- Implantable Cardioverter-Defibrillators for Primary Prevention of Sudden Cardiac Death
