Clin Endosc.
2014 Jul;47(4):367-370. 10.5946/ce.2014.47.4.367.
Electrohydraulic Lithotripsy of an Impacted Enterolith Causing Acute Afferent Loop Syndrome
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Soonchunhyang University Cheonan Hospital, Soonchunhyang University College of Medicine, Cheonan, Korea. thlee9@schmc.ac.kr
- KMID: 1907941
- DOI: http://doi.org/10.5946/ce.2014.47.4.367
Abstract
- Afferent loop syndrome caused by an impacted enterolith is very rare, and endoscopic removal of the enterolith may be difficult if a stricture is present or the normal anatomy has been altered. Electrohydraulic lithotripsy is commonly used for endoscopic fragmentation of biliary and pancreatic duct stones. A 64-year-old man who had undergone subtotal gastrectomy and gastrojejunostomy presented with acute, severe abdominal pain for a duration of 2 hours. Initially, he was diagnosed with acute pancreatitis because of an elevated amylase level and pain, but was finally diagnosed with acute afferent loop syndrome when an impacted enterolith was identified by computed tomography. We successfully removed the enterolith using direct electrohydraulic lithotripsy conducted using a transparent cap-fitted endoscope without complications. We found that this procedure was therapeutically beneficial.
MeSH Terms
Figure
-
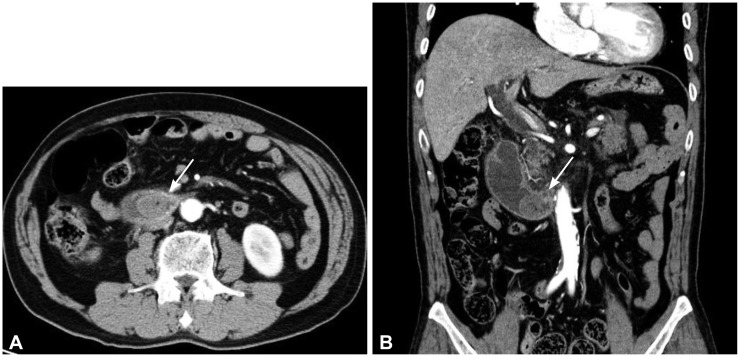
Fig. 1 (A) An axial abdominal computed tomography (CT) image showing a large impacted enterolith (arrow) in the dilated fluid-filled afferent loop. (B) Coronal CT reconstruction better demonstrating the afferent loop obstruction by the enterolith (arrow).

Fig. 2 (A) Endoscopically, an impacted yellow enterolith is apparent in the afferent loop. (B) Contrast material could not pass the obstruction due to the completely impacted enterolith on the fluoroscopic image.

Fig. 3 (A) The enterolith is pulverized via electrohydraulic lithotripsy. (B) The fragmented enterolith after endoscopic removal. (C) A very large ulcerative lesion on a blind pouch of the afferent loop.
Reference
-
1. Jordan GL Jr. Surgical management of postgastrectomy problems. Arch Surg. 1971; 102:251–259. PMID: 5553296.
Article3. Lee MC, Bui JT, Knuttinen MG, Gaba RC, Scott Helton W, Owens CA. Enterolith causing afferent loop obstruction: a case report and literature review. Cardiovasc Intervent Radiol. 2009; 32:1091–1096. PMID: 19365684.
Article4. Kim HJ, Moon JH, Choi HJ, et al. Endoscopic removal of an enterolith causing afferent loop syndrome using electrohydraulic lithotripsy. Dig Endosc. 2010; 22:220–222. PMID: 20642613.
Article5. Carbognin G, Biasiutti C, El-Khaldi M, Ceratti S, Procacci C. Afferent loop syndrome presenting as enterolith after Billroth II subtotal gastrectomy: a case report. Abdom Imaging. 2000; 25:129–131. PMID: 10675451.
Article6. Kim JK, Park CH, Huh JH, et al. Endoscopic management of afferent loop syndrome after a pylorus preserving pancreatoduodenecotomy presenting with obstructive jaundice and ascending cholangitis. Clin Endosc. 2011; 44:59–64. PMID: 22741115.
Article7. Capaccio E, Zuccarino F, Gauglio C, Pretolesi F, Derchi LE. Acute obstruction of the afferent loop caused by an enterolith. Emerg Radiol. 2007; 13:201–203. PMID: 17109128.
Article8. Gale ME, Gerzof SG, Kiser LC, et al. CT appearance of afferent loop obstruction. AJR Am J Roentgenol. 1982; 138:1085–1088. PMID: 6979208.
Article9. Moriura S, Ikeda S, Kimura A, Iwatsuka Y, Ikezawa T, Naiki K. Jaundice due to afferent loop obstruction following hepatectomy for a hilar cholangiocarcinoma. Abdom Imaging. 1996; 21:226–227. PMID: 8661553.
Article10. Moriura S, Takayama Y, Nagata J, et al. Percutaneous bowel drainage for jaundice due to afferent loop obstruction following pancreatoduodenectomy: report of a case. Surg Today. 1999; 29:1098–1101. PMID: 10554338.
Article11. Burdick JS, Garza AA, Magee DJ, Dykes C, Jeyarajah R. Endoscopic management of afferent loop syndrome of malignant etiology. Gastrointest Endosc. 2002; 55:602–605. PMID: 11923786.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous Cholangioscopic Lithotripsy for Afferent Loop Syndrome Caused by Enterolith Development after Roux-en-Y Hepaticojejunostomy: A Case Report
- A Case of Afferent Loop Syndrome with Acute Cholangitis Developed after Percutaneous Transhepatic Cholangioscopic Lithotripsy for Treatment of Choledocholithiasis in a Patient Who Underwent Billroth II Gastrectomy
- Effects of Electrohydraulic Lithotripsy on the Rabbit Bladder According to the Distance
- Acute Abdomen Caused by Complicated Afferent Loop Syndrome after Gastrectomy
- Minimally Invasive Approach Using Digital Single-Operator Peroral Cholangioscopy-Guided Electrohydraulic Lithotripsy and Endoscopic Nasogallbladder Drainage for the Management of High-Grade Mirizzi Syndrome
