Outcome of Surgical Treatment of AO Type C Pelvic Ring Injury
- Affiliations
-
- 1Department of Orthopedic Surgery, Gachon University Gil Medical Center, Incheon, Korea. chlwkdtjr@hanmail.net
- KMID: 1907704
- DOI: http://doi.org/10.5371/hp.2014.26.4.269
Abstract
- PURPOSE
To evaluate the radiologic and clinical outcomes of AO type C pelvic ring injury and identify the prognostic factors.
MATERIALS AND METHODS
We studied 53 patients who were treated for AO type C pelvic ring injury from January 2002 to February 2010. Mean age and mean follow-up duration were 42.4 years and 14 months, respectively. We had 8 cases of AO type C1-1, 19 cases of C1-2, 11 cases of C1-3, 6 cases of C2 and 9 cases of C3 injury. We analyzed type of fracture, displacement, method of fixation and associated injuries. Radiologic outcome was evaluated with Matta and Saucedo criteria and clinical outcome was evaluated using Majeed score.
RESULTS
The average Majeed score was 86.2 distributing as 36 excellent cases, 15 good cases and 2 fair cases. Using radiologic Matta and Saucedo criteria, patients were divided as 31 excellent cases, 17 good cases and 5 fair cases. There was no significant difference between the outcomes of anterior, posterior and antero-posterior fixation. Neurologic injury was the reason for an unsatisfactory functional outcome. We identified two cases with complication, one with postoperative infection and the other with nonunion following anterior-posterior fixation.
CONCLUSION
Satisfactory radiologic and clinical outcomes were obtained with open reduction and internal fixation in the management of AO type C pelvic ring injuries. Neurologic injuries affected the clinical outcome.
MeSH Terms
Figure
-

Fig. 1 A 48-year-old male patient who had AO type C1-3 fractures. (A) Pre-operative pelvis antero-posterior X-ray showed separation of symphysis pubis. (B) Computed tomography scan revealed a sacral fracture of Denis Type II. (C) Symphysis pubis was fixed by a reconstruction plate. (D) After 17 months, the fracture site was united.
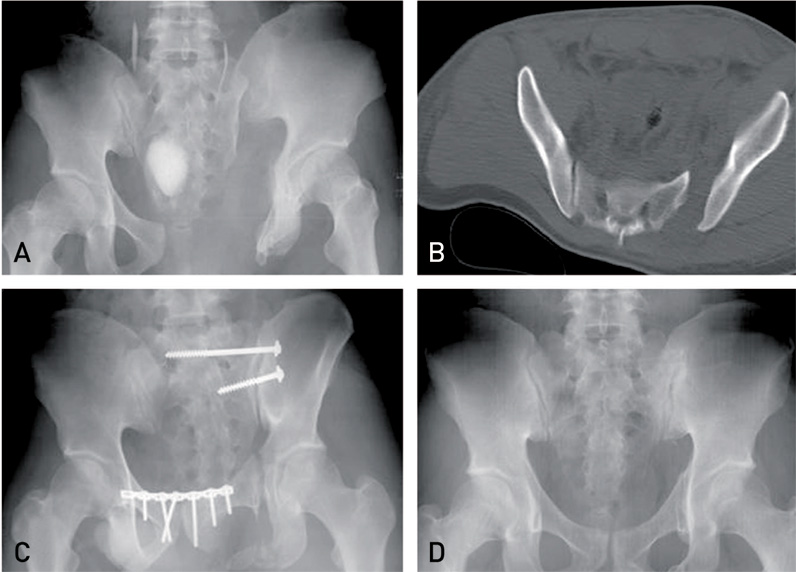
Fig. 2 A 28-year-old male patient who had AO type C1-2 fractures. (A) Pre-operative pelvis antero-posterior X-ray showed symphysis pubis and sacroiliac joint separations. (B) Computed tomography scan revealed a sacroiliac joint separation. (C) Symphysis pubis was fixed by a reconstruction plate and the posterior ring was fixed by a 6.5 mm cancellous screw. (D) After 14 months, metal removal was done and well reduced fracture was observed.
Reference
-
1. Chang JD, Seo YJ, Choi YH. Problems of anterior external fixation in unstable pelvic ring injury. J Korean Fract Soc. 2005; 18:394–398.
Article2. Kim WY, Ji JH, Kim YY, Yang YJ, Lee DY. Anterior fixation techniques on unstable pelvic ring injury. J Korean Orthop Assoc. 2005; 40:8–13.
Article3. Oh CW, Kim PT, Park BC, et al. Anterior plating and iliosacral screwing for unstable pelvic injury. J Korean Orthop Assoc. 2007; 42:483–489.
Article4. Pohlemann T, Bosch U, Gänsslen A, Tscherne H. The Hannover experience in management of pelvic fractures. Clin Orthop Relat Res. 1994; 305:69–80.
Article5. Tile M. Acute pelvic fractures: I. Causation and classification. J Am Acad Orthop Surg. 1996; 4:143–151.
Article6. Lindahl J, Hirvensalo E. Outcome of operatively treated type-C injuries of the pelvic ring. Acta Orthop. 2005; 76:667–678.
Article7. Oh KJ, Hwang SM. Surgical fixation of sacroiliac joint complex in unstable pelvic ring injuries. Hip Pelvis. 2012; 24:139–147.
Article8. Kim JJ, Kim JW, Chang JS. Clinical outcome of AO type C pelvic ring injury. J Korean Orthop Assoc. 2005; 40:181–187.
Article9. Min BW, Kang CH, Shin HK. Complication of the operative treatment in unstable pelvic bone fractures. J Korean Hip Soc. 2004; 16:373–379.10. Matta JM, Saucedo T. Internal fixation of pelvic ring fractures. Clin Orthop Relat Res. 1989; 242:83–97.
Article11. Majeed SA. Grading the outcome of pelvic fractures. J Bone Joint Surg Br. 1989; 71:304–306.
Article12. Matta JM. Indications for anterior fixation of pelvic fractures. Clin Orthop Relat Res. 1996; 329:88–96.
Article13. Lindahl J, Hirvensalo E, Böstman O, Santavirta S. Failure of reduction with an external fixator in the management of injuries of the pelvic ring. Long-term evaluation of 110 patients. J Bone Joint Surg Br. 1999; 81:955–962.14. Patterson FP, Morton KS. Neurological complications of fractures and dislocations of the pelvis. J Trauma. 1972; 12:1013–1023.
Article15. Kutsy RL, Robinson LR, Routt ML Jr. Lumbosacral plexopathy in pelvic trauma. Muscle Nerve. 2000; 23:1757–1760.
Article16. Lee SH, Ha SH, Lee YK, Cho SW, Park SS. Operative treatment of unstable pelvic ring injury. J Korean Fract Soc. 2012; 25:243–249.
Article17. Tornetta P 3rd, Dickson K, Matta JM. Outcome of rotationally unstable pelvic ring injuries treated operatively. Clin Orthop Relat Res. 1996; 329:147–151.
Article
