Recurrent Cardioembolic Stroke Treated Successfully with Repeated Mechanical Thrombectomy within the Acute Index Stroke Period
- Affiliations
-
- 1Department of Neurology, Yonsei University College of Medicine, Seoul, Korea. neuro05@yuhs.ac
- 2Department of Radiology, Yonsei University College of Medicine, Seoul, Korea.
- 3Department of Pathology, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1894568
- DOI: http://doi.org/10.3988/jcn.2015.11.3.275
Abstract
- BACKGROUND
The safety of repeated mechanical thrombectomy within the acute stroke period has not yet been clearly demonstrated. We describe herein a patient who was successfully treated with repeated mechanical thrombectomy within the acute index stroke period.
CASE REPORT
A 50-year-old woman with atrial fibrillation presented with left-sided weakness caused by occlusion of the right middle cerebral artery (MCA). Emergent mechanical thrombectomy with the Solitaire device achieved complete recanalization. The left MCA occlusion redeveloped at 6 days after the first treatment, at which time her international normalized ratio (INR) was 2.3. Endovascular thrombectomy was reattempted rapidly and complete recanalization was achieved again. Her neurologic symptoms resolved after the thrombectomy.
CONCLUSIONS
This case demonstrates that repeated mechanical thrombectomy can be safely and successfully performed even in a patient with a high INR and a recurrent stroke during the acute period after the index stroke.
Keyword
MeSH Terms
Figure
-
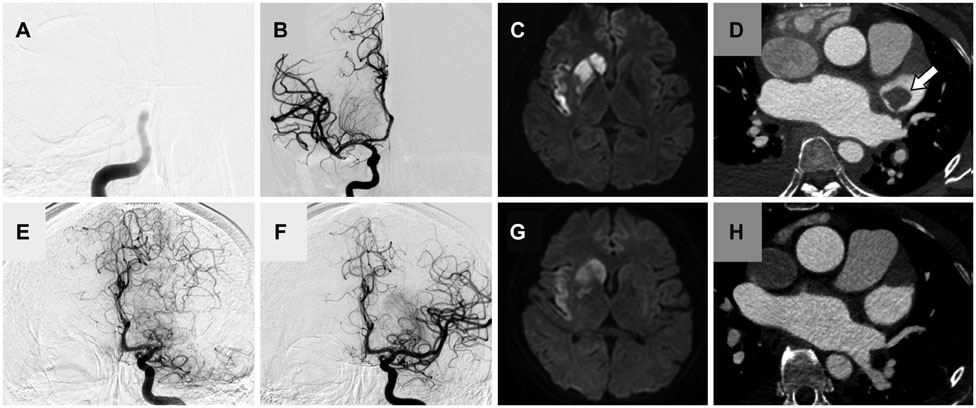
Fig. 1 Digital subtraction angiography (DSA), brain MRI, and coronary computed tomography (CT) of the patient. A: Initial DSA showing thromboembolic occlusion of the right distal internal carotid artery (ICA). B: Mechanical thrombectomy with the Solitaire (ev3 Inc.) device against the right distal ICA and middle cerebral artery (MCA), which achieved complete recanalization. C: Diffusion-weighted MRI revealing an acute infarction in the right insula and basal ganglia. D: Coronary CT demonstrating a 22-mm-sized thrombus (white arrow) in the left atrial appendage. E: The patient suffered a second stroke 6 days after the index stroke; DSA revealing embolic occlusion of the left proximal MCA. F: The left MCA was successfully reopened after mechanical thrombectomy using the suction thrombectomy and Solitaire (ev3 Inc.) devices. G: Follow-up diffusion-weighted MRI revealing a slightly increased signal intensity in the left basal ganglia. H: Follow-up coronary CT after the second stroke confirming disappearance of the thrombus in the heart.
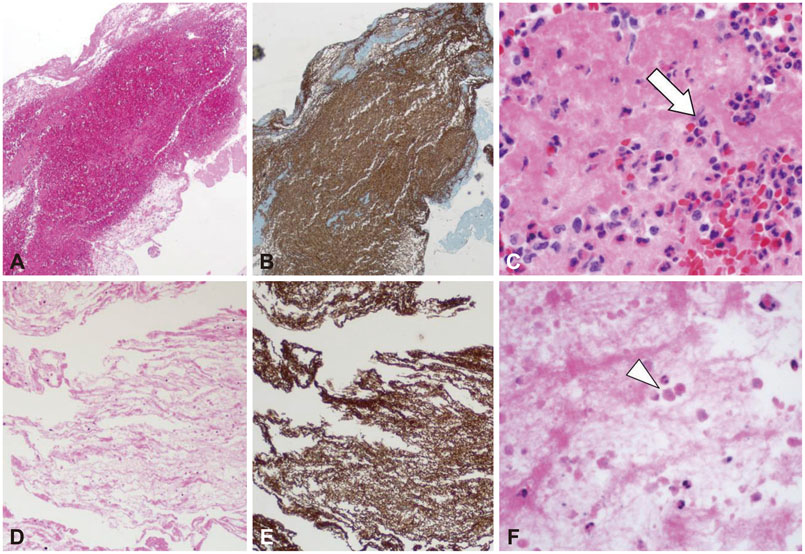
Fig. 2 Hematoxylin and eosin staining (original magnification ×40). (A) The extracted thrombus from the index stroke exhibited a large number of red blood cells (RBCs), whereas (D) the clot extracted from the second stroke appeared to have fewer RBCs and a larger amount of fibrin. However, antiglycophorin-A staining (original magnification ×40) revealed that the thrombus extracted following the first (B) and second (E) strokes were erythrocyte-rich thrombi. (C) Detail of panel A showing intact RBCs and granulocytes (white arrow). (F) Detail of panel D revealing degraded RBCs and granulocyte apoptosis (white arrowhead).
Reference
-
1. Layton KF, White JB, Cloft HJ, Kallmes DF, Manno EM. Expanding the treatment window with mechanical thrombectomy in acute ischemic stroke. Neuroradiology. 2006; 48:402–404.
Article2. Nogueira RG, Smith WS. MERCI and Multi MERCI Writing Committee. Safety and efficacy of endovascular thrombectomy in patients with abnormal hemostasis: pooled analysis of the MERCI and multi MERCI trials. Stroke. 2009; 40:516–522.
Article3. Nogueira RG, Yoo AJ, Buonanno FS, Hirsch JA. Endovascular approaches to acute stroke, part 2: a comprehensive review of studies and trials. AJNR Am J Neuroradiol. 2009; 30:859–875.
Article4. Nogueira RG, Schwamm LH, Hirsch JA. Endovascular approaches to acute stroke, part 1: Drugs, devices, and data. AJNR Am J Neuroradiol. 2009; 30:649–661.
Article5. Koh JS, Lee SJ, Ryu CW, Kim HS. Safety and efficacy of mechanical thrombectomy with solitaire stent retrieval for acute ischemic stroke: a systematic review. Neurointervention. 2012; 7:1–9.
Article6. Smith WS, Sung G, Saver J, Budzik R, Duckwiler G, Liebeskind DS, et al. Mechanical thrombectomy for acute ischemic stroke: final results of the Multi MERCI trial. Stroke. 2008; 39:1205–1212.7. Willinsky RA, Taylor SM, TerBrugge K, Farb RI, Tomlinson G, Montanera W. Neurologic complications of cerebral angiography: prospective analysis of 2,899 procedures and review of the literature. Radiology. 2003; 227:522–528.
Article8. Arboix A, Alió J. Cardioembolic stroke: clinical features, specific cardiac disorders and prognosis. Curr Cardiol Rev. 2010; 6:150–161.
Article9. Bernhardt P, Schmidt H, Hammerstingl C, Lüderitz B, Omran H. Atrial thrombi-a prospective follow-up study over 3 years with transesophageal echocardiography and cranial magnetic resonance imaging. Echocardiography. 2006; 23:388–394.
Article10. Rittersma SZ, van der Wal AC, Koch KT, Piek JJ, Henriques JP, Mulder KJ, et al. Plaque instability frequently occurs days or weeks before occlusive coronary thrombosis: a pathological thrombectomy study in primary percutaneous coronary intervention. Circulation. 2005; 111:1160–1165.
Article11. Taborelli A, Andreola S, Di Giancamillo A, Gentile G, Domeneghini C, Grandi M, et al. The use of the anti-Glycophorin A antibody in the detection of red blood cell residues in human soft tissue lesions decomposed in air and water: a pilot study. Med Sci Law. 2011; 51:Suppl 1. S16–S19.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Mechanical Thrombectomy with Solitaire Stent Retrieval for Acute Cardioembolic Stroke
- Acute Ischemic Stroke in a 6-Year-Old Boy, Treated with Mechanical Thrombectomy: A Case Report
- Differences in Effectiveness among Devices for Endovascular Thrombectomy in Patients with Acute Ischemic Stroke
- Endovascular Treatment of Acute Ischemic Stroke
- Risk Factors for Acute Cardioembolic Brain Stroke in Acute Myocardial Infarction
