A comparison between surgical resection and radiofrequency ablation in the treatment of hepatocellular carcinoma
- Affiliations
-
- 1Division of Hepatico-Biliary-Pancreatic Surgery, Department of Surgery, Chonnam National University Medical School, Gwangju, Korea. ckcho@jnu.ac.kr
- 2Department of Radiology, Chonnam National University Medical School, Gwangju, Korea.
- KMID: 1882834
- DOI: http://doi.org/10.4174/astr.2014.87.2.72
Abstract
- PURPOSE
The aim of this study was to compare the therapeutic effects of radiofrequency ablation (RFA) and hepatic resection (HR) with regards to procedural morbidity, mortality, overall survival (OS) and disease-free survival (DFS) rates in hepatocellular carcinoma (HCC) patients.
METHODS
Retrospective studies were performed based on the medical records of 129 patients who underwent curative HR, and 57 who patients received RFA for HCC, between 2005 and 2009. The inclusion criteria of HCC were the presence of three or fewer nodules 3 cm or less in diameter or a single nodule of 5 cm or less.
RESULTS
The 1-, 3- and 5-year OS rates in the HR group were 91.3%, 78.8%, and 64.9%, compared to 94.4%, 74.0%, and 74.0% in the RFA group, with no significant difference between the two groups (P = 0.725). The estimated 1- and 3-year DFS rates were 70.0% and 53.0% in the HR group and 65.2% and 24.7% in the RFA group, respectively. The DFS rates of HR group were significantly higher than RFA group (P = 0.015). Multivariate analysis identified that recurrence (P = 0.036) and portal hypertension (P = 0.036) were associated with OS and that portal hypertension (P = 0.048) and increased serum alpha-FP (P = 0.008) were the factors significantly associated with DFS.
CONCLUSION
HCC within Milan criteria should consider hepatectomy as the primary treatment if the patient's liver function and general conditions are good enough to undergo surgical operation. But in that RFA revealed similar overall survival to HR, RFA can be an alternative therapy for patients who are eligible for surgical resection.
MeSH Terms
Figure
-
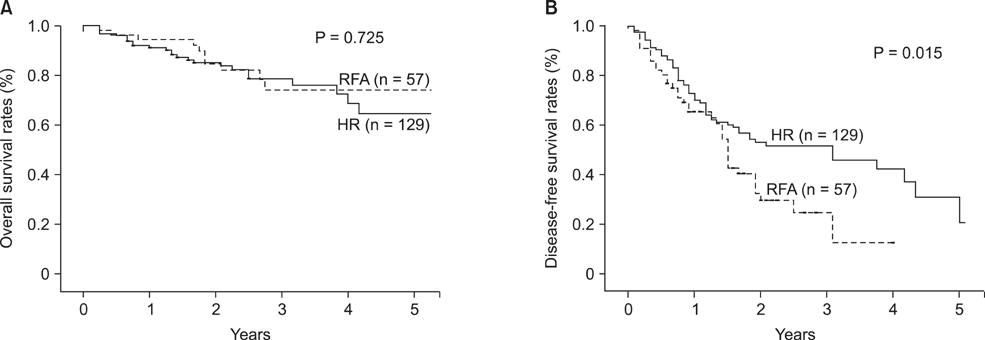
Fig. 1 Overall (A) and disease-free survival (B) of all patients in the two treatment groups. (A) The overall survival were not significantly different (P = 0.725), in the two treatment groups. (B) But disease-free survival was significantly higher in hepatic resection (HR) group (P = 0.015). RFA, radiofrequency ablation.

Fig. 2 Disease-free survival of patients with hepatocellular carcinoma (HCC ≤ 3 cm (A) and 3 cm < HCC ≤ 5 cm (B) in the two treatment groups. (A) Disease-free survival was significantly higher in resection group (P = 0.003). (B) Disease-free survival was higher in hepatic resection (HR) group but the difference did not reach statistical significance (P = 0.099). RFA, radiofrequency ablation.

Fig. 3 Disease-free survival of patients with α-FP below 20 ng/mL and absence of portal hypertension in the two treatment groups: Disease-free survival was higher in hepatic resection (HR) group but the difference did not reach statistical significance (P = 0.228). RFA, radiofrequency ablation.
Cited by 1 articles
-
Long-term Survival in Patients Treated with a Robotic Radiosurgical Device for Liver Metastases
Sebastian Stintzing, Jobst von Einem, Christoph Fueweger, Alfred Haidenberger, Michael Fedorov, Alexander Muavcevic
Cancer Res Treat. 2019;51(1):187-193. doi: 10.4143/crt.2017.594.
Reference
-
1. Bosch FX, Ribes J, Borras J. Epidemiology of primary liver cancer. Semin Liver Dis. 1999; 19:271–285.2. Ministry of Health & Welfare. Annual report of cancer incidence (2005) and survival (1993-2005) in Korea. Seoul: Ministry of Health & Welfare;2008.3. Bosch FX, Ribes J, Cleries R, Diaz M. Epidemiology of hepatocellular carcinoma. Clin Liver Dis. 2005; 9:191–211. v4. Bruix J, Sherman M, Llovet JM, Beaugrand M, Lencioni R, Burroughs AK, et al. European Association for the Study of the Liver. Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. J Hepatol. 2001; 35:421–430.5. Livraghi T. Guidelines for treatment of liver cancer. Eur J Ultrasound. 2001; 13:167–176.6. Marin-Hargreaves G, Azoulay D, Bismuth H. Hepatocellular carcinoma: surgical indications and results. Crit Rev Oncol Hematol. 2003; 47:13–27.7. Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996; 334:693–699.8. Margarit C, Escartin A, Castells L, Vargas V, Allende E, Bilbao I. Resection for hepatocellular carcinoma is a good option in Child-Turcotte-Pugh class A patients with cirrhosis who are eligible for liver transplantation. Liver Transpl. 2005; 11:1242–1251.9. Zhou XD, Tang ZY, Yang BH, Lin ZY, Ma ZC, Ye SL, et al. Experience of 1000 patients who underwent hepatectomy for small hepatocellular carcinoma. Cancer. 2001; 91:1479–1486.10. Liver Cancer Study Group of Japan. Primary liver cancer in Japan. Clinicopathologic features and results of surgical treatment. Ann Surg. 1990; 211:277–287.11. Lai EC, Fan ST, Lo CM, Chu KM, Liu CL, Wong J. Hepatic resection for hepatocellular carcinoma: an audit of 343 patients. Ann Surg. 1995; 221:291–298.12. Fan ST, Lo CM, Liu CL, Lam CM, Yuen WK, Yeung C, et al. Hepatectomy for hepatocellular carcinoma: toward zero hospital deaths. Ann Surg. 1999; 229:322–330.13. Fong Y, Sun RL, Jarnagin W, Blumgart LH. An analysis of 412 cases of hepatocellular carcinoma at a Western center. Ann Surg. 1999; 229:790–799.14. Livraghi T. Radiofrequency ablation, PEIT, and TACE for hepatocellular carcinoma. J Hepatobiliary Pancreat Surg. 2003; 10:67–76.15. Livraghi T, Goldberg SN, Lazzaroni S, Meloni F, Solbiati L, Gazelle GS. Small hepatocellular carcinoma: treatment with radio-frequency ablation versus ethanol injection. Radiology. 1999; 210:655–661.16. Ikeda M, Okada S, Ueno H, Okusaka T, Kuriyama H. Radiofrequency ablation and percutaneous ethanol injection in patients with small hepatocellular carcinoma: a comparative study. Jpn J Clin Oncol. 2001; 31:322–326.17. Lencioni RA, Allgaier HP, Cioni D, Olschewski M, Deibert P, Crocetti L, et al. Small hepatocellular carcinoma in cirrhosis: randomized comparison of radio-frequency thermal ablation versus percutaneous ethanol injection. Radiology. 2003; 228:235–240.18. Hong SN, Lee SY, Choi MS, Lee JH, Koh KC, Paik SW, et al. Comparing the outcomes of radiofrequency ablation and surgery in patients with a single small hepatocellular carcinoma and well-preserved hepatic function. J Clin Gastroenterol. 2005; 39:247–252.19. Livraghi T, Meloni F, Di Stasi M, Rolle E, Solbiati L, Tinelli C, et al. Sustained complete response and complications rates after radiofrequency ablation of very early hepatocellular carcinoma in cirrhosis: Is resection still the treatment of choice? Hepatology. 2008; 47:82–89.20. Korean Liver Cancer Study Group and National Cancer Center, Korea. Practice guidelines for management of hepatocellular carcinoma 2009. Korean J Hepatol. 2009; 15:391–423.21. Bruix J, Sherman M. Practice Guidelines Committee, American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma. Hepatology. 2005; 42:1208–1236.22. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004; 240:205–213.23. Chen MH, Yang W, Yan K, Zou MW, Solbiati L, Liu JB, et al. Large liver tumors: protocol for radiofrequency ablation and its clinical application in 110 patients: mathematic model, overlapping mode, and electrode placement process. Radiology. 2004; 232:260–271.24. Colombo M, de Franchis R, Del Ninno E, Sangiovanni A, De Fazio C, Tommasini M, et al. Hepatocellular carcinoma in Italian patients with cirrhosis. N Engl J Med. 1991; 325:675–680.25. El-Serag HB, Mason AC. Rising incidence of hepatocellular carcinoma in the United States. N Engl J Med. 1999; 340:745–750.26. Chen MS, Li JQ, Zheng Y, Guo RP, Liang HH, Zhang YQ, et al. A prospective randomized trial comparing percutaneous local ablative therapy and partial hepatectomy for small hepatocellular carcinoma. Ann Surg. 2006; 243:321–328.27. Ueno S, Sakoda M, Kubo F, Hiwatashi K, Tateno T, Baba Y, et al. Surgical resection versus radiofrequency ablation for small hepatocellular carcinomas within the Milan criteria. J Hepatobiliary Pancreat Surg. 2009; 16:359–366.28. Ueno S, Tanabe G, Nuruki K, Oketani M, Komorizono Y, Hokotate H, et al. Prognosis of hepatocellular carcinoma associated with Child class B and C cirrhosis in relation to treatment: a multivariate analysis of 411 patients at a single center. J Hepatobiliary Pancreat Surg. 2002; 9:469–477.29. Mulier S, Ni Y, Jamart J, Ruers T, Marchal G, Michel L. Local recurrence after hepatic radiofrequency coagulation: multivariate meta-analysis and review of contributing factors. Ann Surg. 2005; 242:158–171.30. Ng KK, Poon RT, Lo CM, Yuen J, Tso WK, Fan ST. Analysis of recurrence pattern and its influence on survival outcome after radiofrequency ablation of hepatocellular carcinoma. J Gastrointest Surg. 2008; 12:183–191.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Radiofrequency Thermal Ablation of Hepatocellular Carcinomas
- Surgical resection versus ablation for early hepatocellular carcinoma: The debate is still open
- Current status and future of radiofrequency ablation for hepatocellular carcinoma
- Chemoembolization combined with radiofrequency ablation is the best option for the local treatment of early hepatocellular carcinoma?
- Microwave thermosphere versus radiofrequency ablation for hepatocellular carcinoma: Are we approaching the time to end the debate?
