A Case of Occupational Hypersensitivity Pneumonitis Associated with Trichloroethylene
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. chungks@yuhs.ac
- 2The Institute of Chest Disease, Yonsei University College of Medicine, Seoul, Korea.
- 3Department of Pathology, Yonsei University College of Medicine, Seoul, Korea.
- 4Department of Thoracic Surgery, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1877344
- DOI: http://doi.org/10.4046/trd.2014.76.2.75
Abstract
- Trichloroethylene (TCE) is a toxic chemical commonly used as a degreasing agent, and it is usually found in a colorless or blue liquid form. TCE has a sweet, chloroform-like odor, and this volatile chlorinated organic chemical can cause toxic hepatitis, neurophysiological disorders, skin disorders, and hypersensitivity syndromes. However, the hypersensitivity pneumonitis (HP) attributed to TCE has rarely been reported. We hereby describe a case of HP associated with TCE in a 29-year-old man who was employed as a lead welder at a computer repair center. He was installing the capacitors on computer chip boards and had been wiped down with TCE. He was admitted to our hospital with complaints of dry coughs, night sweats, and weight losses for the past two months. HP due to TCE exposure was being suspected due to his occupational history, and the results of a video-associated thoracoscopic biopsy confirmed the suspicions. Symptoms have resolved after the steroid pulse therapy and his occupational change. TCE should be taken into consideration as a potential trigger of HP. Early recognition and avoidance of the TCE exposure in the future is important for the treatment of TCE induced HP.
MeSH Terms
Figure
-

Figure 1 (A) Chest X-ray: some reticulonodular densities on both upper lobes. (B) Pulmonary function test: forced vital capacity (FVC) 4.58 L (90% ref), forced expiratory volume in 1 second (FEV1) 3.87 L (91% ref), FEV1/FVC 84%, FEF25-65% 3.61 L/sec (82% ref), DLCO 23.1 mL/mm Hg/min (83% ref). TLC: total lung capacity; ERV: expiratory reserve volume; RV: residual volume.

Figure 2 Tiny ill-defined nodules, predominant on both upper lobes, suggestive of hypersensitivity pneumonitis.

Figure 3 Multifocal patchy young fibroblastic proliferation, chronic inflammatory cell infiltration around respiratory bronchiole associated with foamy histiocytic aggregations (H&E stain, ×100).
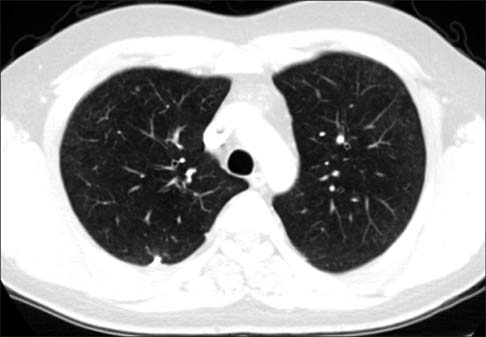
Figure 4 Near complete resolution.
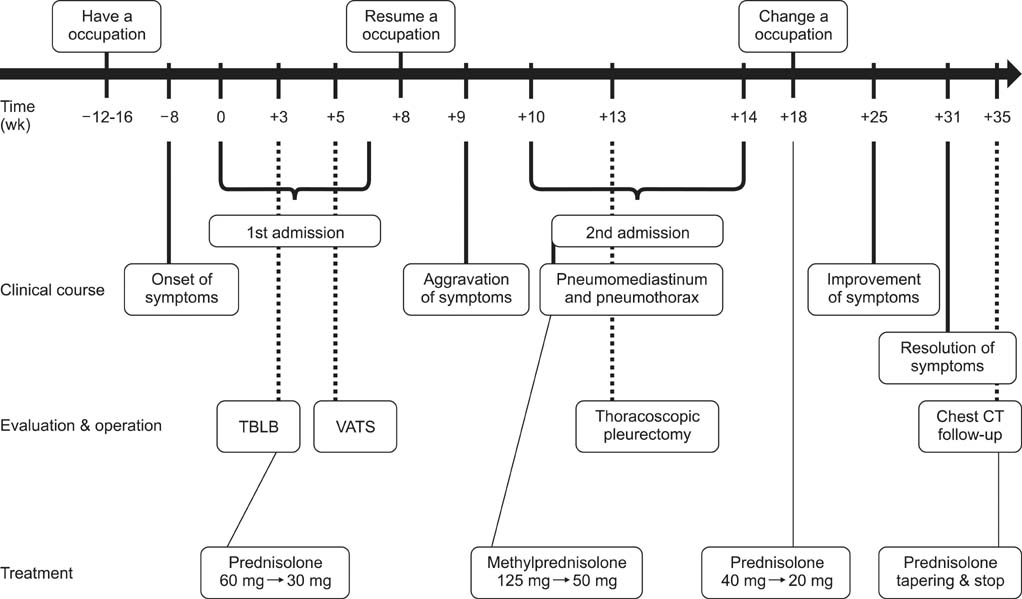
Figure 5 Outline of the clinical course and treatment. TBLB: transbronchial lung biopsy; VATS: video-associated thoracoscopy; CT: computed tomography.
Cited by 1 articles
-
Late-onset trichloroethylene-induced hypersensitivity syndrome after intermittent exposure to low-dose trichloroethylene
Seung Yun Lee, Se Hwan Oh, Hyuck Jae Choi, Woo Young Choi, Jee Young Han, Hong-Lyeol Lee, Cheol-Woo Kim
Allergy Asthma Respir Dis. 2016;4(2):145-148. doi: 10.4168/aard.2016.4.2.145.
Reference
-
1. Bakke B, Stewart PA, Waters MA. Uses of and exposure to trichloroethylene in U.S. industry: a systematic literature review. J Occup Environ Hyg. 2007; 4:375–390.2. Tanios MA, El Gamal H, Rosenberg BJ, Hassoun PM. Can we still miss tetrachloroethylene-induced lung disease? The emperor returns in new clothes. Respiration. 2004; 71:642–645.3. Hansen J, Sallmen M, Selden AI, Anttila A, Pukkala E, Andersson K, et al. Risk of cancer among workers exposed to trichloroethylene: analysis of three Nordic cohort studies. J Natl Cancer Inst. 2013; 105:869–877.4. Parker JC, Bahlman LJ, Leidel NA, Stein HP, Thomas AW, Wolf BS, et al. Current NIOSH Intelligence Bulletin No. 20: tetrachloroethylene (perchloroethylene). Am Ind Hyg Assoc J. 1978; 39:A-23–A-29.5. Pastino GM, Yap WY, Carroquino M. Human variability and susceptibility to trichloroethylene. Environ Health Perspect. 2000; 108:Suppl 2. 201–214.6. Kamijima M, Hisanaga N, Wang H, Nakajima T. Occupational trichloroethylene exposure as a cause of idiosyncratic generalized skin disorders and accompanying hepatitis similar to drug hypersensitivities. Int Arch Occup Environ Health. 2007; 80:357–370.7. Goon AT, Lee LT, Tay YK, Yosipovitch G, Ng SK, Giam YC. A case of trichloroethylene hypersensitivity syndrome. Arch Dermatol. 2001; 137:274–276.8. Schuyler M, Cormier Y. The diagnosis of hypersensitivity pneumonitis. Chest. 1997; 111:534–536.9. Jacobs RL, Andrews CP, Coalson JJ. Hypersensitivity pneumonitis: beyond classic occupational disease-changing concepts of diagnosis and management. Ann Allergy Asthma Immunol. 2005; 95:115–128.10. Lacasse Y, Selman M, Costabel U, Dalphin JC, Ando M, Morell F, et al. Clinical diagnosis of hypersensitivity pneumonitis. Am J Respir Crit Care Med. 2003; 168:952–958.11. Tanaka H, Tsunematsu K, Nakamura N, Suzuki K, Tanaka N, Takeya I, et al. Successful treatment of hypersensitivity pneumonitis caused by Grifola frondosa (Maitake) mushroom using a HFA-BDP extra-fine aerosol. Intern Med. 2004; 43:737–740.12. Tong Z, Chen B, Dai H, Bauer PC, Guzman J, Costabel U. Extrinsic allergic alveolitis: inhibitory effects of pentoxifylline on cytokine production by alveolar macrophages. Ann Allergy Asthma Immunol. 2004; 92:234–239.13. Churg A, Muller NL, Flint J, Wright JL. Chronic hypersensitivity pneumonitis. Am J Surg Pathol. 2006; 30:201–208.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Trichloroethylene Hypersensitivity Syndrome
- A Study on the Neuropsychiatric Symptom and Neurobehavioral Effects of Occupational Exposure to Trichloroethylene
- Trichloroethylene Hypersensitivity Syndrome: A Disease of Fatal Outcome
- Late-onset trichloroethylene-induced hypersensitivity syndrome after intermittent exposure to low-dose trichloroethylene
- Exfoliative Dermatitis and Toxic Hepatitis Associated with Occupational Exposure to Trichloroethylene
