Obstet Gynecol Sci.
2014 Jul;57(4):338-341. 10.5468/ogs.2014.57.4.338.
Acute abdomen due to ovarian congestion caused by coiling of the fallopian tube accompanied by paratubal cyst around the utero-ovarian ligament
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Gangnam CHA Hospital, CHA University, Seoul, Korea. yspark0108@empas.com
- 2Department of Obstetrics and Gynecology, Bundang CHA Hospital, CHA University, Seongnam, Korea.
- 3Department of Nursing, Saekyung College, Yeongwol, Korea.
- KMID: 1841549
- DOI: http://doi.org/10.5468/ogs.2014.57.4.338
Abstract
- Torsion of uterine adnexa is an important cause of acute abdominal pain in females. The main organ which can cause torsion is the ovaries, but torsions of the fallopian tube, subserosal myoma, paratubal cyst, and even the uterine body have been reported. The incidence of isolated fallopian tubal torsion is very rare. Even more rarely, it can coil around nearby organs such as the utero-ovarian ligament, showing similar clinical manifestations with those of adnexal torsion. We experienced an extremely rare case of acute abdomen induced by ovarian congestion triggered by the fallopian tube accompanying a paratubal cyst coiling around the utero-ovarian ligament. The right paratubal cyst was misinterpreted as being part of a cystic component of the left ovary on preoperative sonographic examination, and the coiling of the right fallopian tube accompanying the paratubal cyst was misdiagnosed as torsion of the right ovary. We report this rare case with a brief literature review.
Keyword
MeSH Terms
Figure
-

Fig. 1 (A) Uterus and right ovary. (B) Detailed view of right ovary (80×32 mm). (C) Left ovary (74×42 mm) and paratubal cyst (67×42 mm).
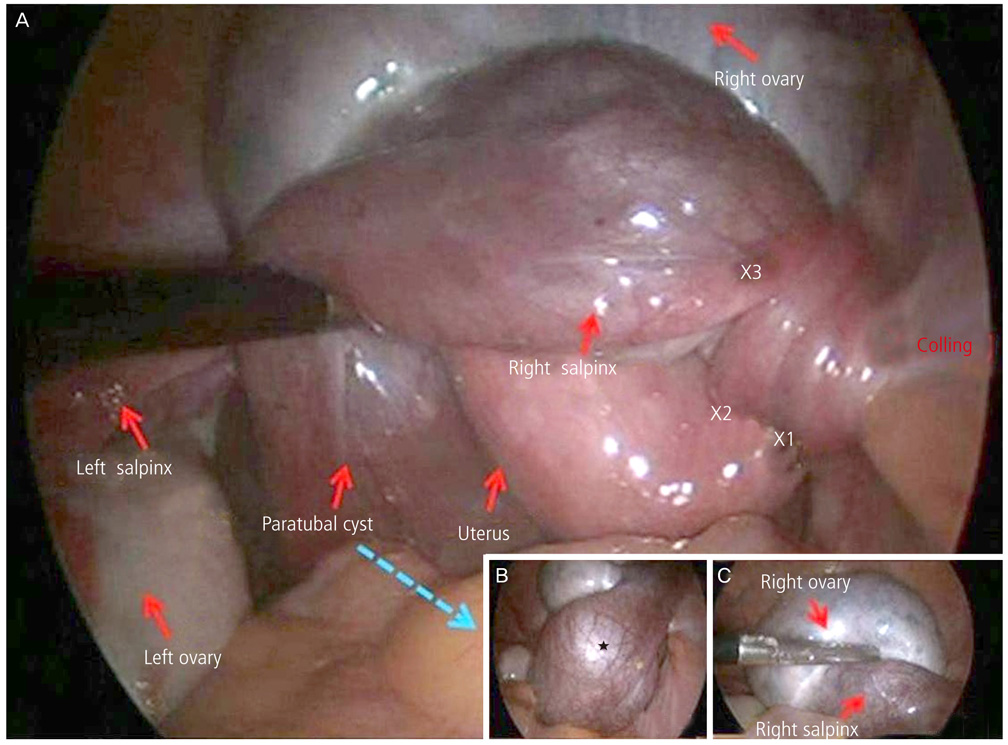
Fig. 2 (A) Laparoscopic view shows right salpinx accompanying with paratubal cyst coiled utero-ovarian ligament 2.5 times, enlarged right ovary situated on the uterus, and paratubal cyst in the cul-de-sac. (B) Left fallopian tube and paratubal cyst. Right fallopian tube and paratubal cyst (★). (C) Right ovary and right fallopian tube.
Reference
-
1. Bransilver BR, Ferenczy A, Richart RM. Female genital tract remnants: an ultrastructural comparison of hydatid of Morgagni and mesonephric ducts and tubules. Arch Pathol. 1973; 96:255–261.2. Gardner GH, Greene RR, Peckham BM. Normal and cystic structures of the broad ligament. Am J Obstet Gynecol. 1948; 55:917–939.3. Athey PA, Cooper NB. Sonographic features of parovarian cysts. AJR Am J Roentgenol. 1985; 144:83–86.4. Hansen OH. Isolated torsion of the Fallopian tube. Acta Obstet Gynecol Scand. 1970; 49:3–6.5. Kaido Y, Kikuchi A, Kanasugi T, Fukushima A, Sugiyama T. Acute abdomen due to ovarian congestion: a fallopian tube accompanied by a paratubal cyst, coiling tightly round the ovary. J Obstet Gynaecol Res. 2013; 39:402–405.6. Valsky DV, Cohen SM, Hamani Y, Lipschuetz M, Yagel S, Esh-Broder E. Whirlpool sign in the diagnosis of adnexal torsion with atypical clinical presentation. Ultrasound Obstet Gynecol. 2009; 34:239–242.7. Krissi H, Shalev J, Bar-Hava I, Langer R, Herman A, Kaplan B. Fallopian tube torsion: laparoscopic evaluation and treatment of a rare gynecological entity. J Am Board Fam Pract. 2001; 14:274–277.
