A Case of Unusual Visceral Heterotaxy Syndrome with Isolated Levocardia
- Affiliations
-
- 1Department of Pediatrics, Chonbuk National University Medical School, Jeonju, Korea. joocu@chonbuk.ac.kr
- 2Institute of Cardiovascular Research, Chonbuk National University Medical School, Jeonju, Korea.
- KMID: 1826564
- DOI: http://doi.org/10.4070/kcj.2013.43.10.705
Abstract
- Situs inversus of the abdominal organs in the presence of normally placed heart on the left side of the thorax is known as situs inversus with isolated levocardia. This rare condition is commonly associated with severe congenital defects of the heart. We report a case of situs inversus with levocardia in a 19-year-old asymptomatic male patient with completely normal heart on the left chest. Spiral computed tomography of the thorax and abdomen and echocardiographic studies revealed situs inversus of abdominal organs, normal heart (levocardia), mirrored left lungs, a midline liver, a left-sided inferior vena cava connecting to the right atrium, multiple splenic masses in the abdominal right upper quadrant, and aneurysmal dilatation of a splenic artery.
Keyword
MeSH Terms
Figure
-

Fig. 1 Chest and abdomen plain X-rays reveal a normally located heart (A) and a right-sided stomach gas shadow, which is displaced by the bridging liver and is not directly beneath the diaphragm (B).
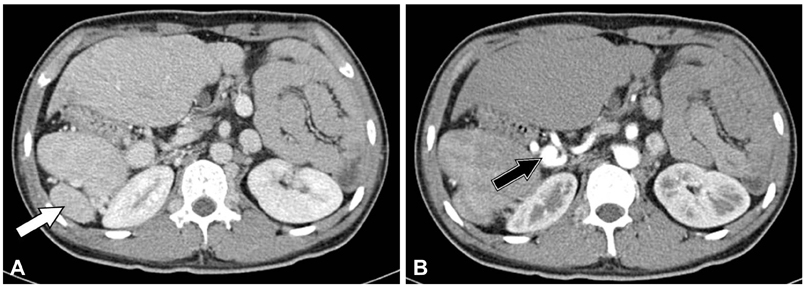
Fig. 2 Spiral computed tomography of the abdomen show situs inversus and multiple spleens (white arrow) in the right upper quadrant (A), and aneurysmal dilatation (black arrow) of a splenic artery (B).

Fig. 3 Hepatic veins (empty arrowheads) show unusual drainage into the inferior vena cava (solid arrowheads); the left hepatic vein (A) into the left-sided inferior vena cava, mid-hepatic veins (B) into inferior vena cava crossing the midline, and the right hepatic vein (C) into the inferior vena cava just before the right atrium.

Fig. 4 The inferior vena cava (solid arrowheads) runs on the left side (A), and the suprahepatic segment of inferior vena cava returns to the right atrium directly (B).
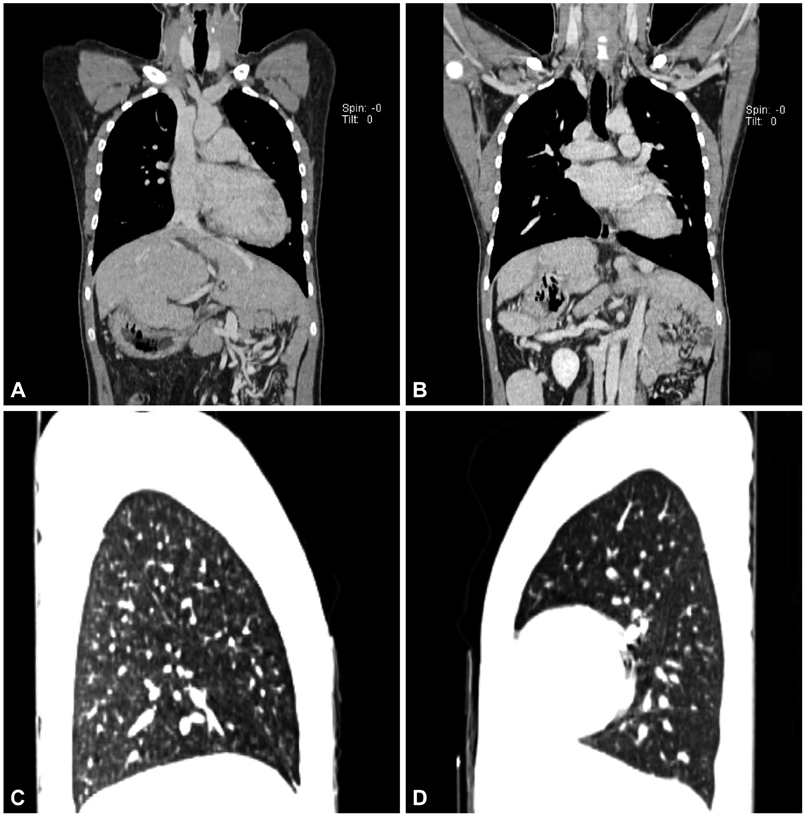
Fig. 5 Spiral computed tomography of the thorax and abdomen demonstrated normal positioning of the ascending aorta, the main pulmonary artery and the superior vena cava (A and B). Sagittal images in lung window setting, right lung (C) shows the mirror structure of the bi-lobed normal left lung (D).
Reference
-
1. Liberthson RR, Hastreiter AR, Sinha SN, Bharati S, Novak GM, Lev M. Levocardia with visceral heterotaxy--isolated levocardia: pathologic anatomy and its clinical implications. Am Heart J. 1973; 85:40–54.2. Gindes L, Hegesh J, Barkai G, Jacobson JM, Achiron R. Isolated levocardia: prenatal diagnosis, clinical importance, and literature review. J Ultrasound Med. 2007; 26:361–365.3. Moller JH, Nakib A, Anderson RC, Edwards JE. Congenital cardiac disease associated with polysplenia. A developmental complex of bilateral "left-sidedness". Circulation. 1967; 36:789–799.4. Rose V, Izukawa T, Moës CA. Syndromes of asplenia and polysplenia. A review of cardiac and non-cardiac malformations in 60 cases withspecial reference to diagnosis and prognosis. Br Heart J. 1975; 37:840–852.5. Imamura T, Momoi N, Go H, Ogasawara K, Sato M, Hosoya M. Rare case of isolated levocardia with polysplenia including normally structured lung without cardiac anomaly. Congenit Anom (Kyoto). 2011; 51:187–190.6. Van Praagh R, Weinberg PM, Smith SD, Foran RB, Van Praagh S. Malposition of the heart. In : Adams FH, Emmanouilides GC, Riemenschneider TA, editors. Moss' Heart Disease in Infants, Children and Adolescents. 4th ed. Baltimore: Williams & Wilkins;1989. p. 530–580.7. O'Leary PW, Hagler DJ. Cardiac malpositions and abnormalities of atrial and visceral situs. In : Allen HD, Driscoll DJ, Shaddy RE, Feltes TF, editors. Moss and Adams' Heart Disease in Infants, Children, and Adolescents. 8th ed. Philadelphia: Lippincott Williams & Wilkins;2013. p. 1207.8. Applegate KE, Goske MJ, Pierce G, Murphy D. Situs revisited: imaging of the heterotaxy syndrome. Radiographics. 1999; 19:837–852. discussion 853-4.9. Peoples WM, Moller JH, Edwards JE. Polysplenia: a review of 146 cases. Pediatr Cardiol. 1983; 4:129–137.10. De La Villeon B, Le Goudeveze S, Goudard Y, Fondin M, Vauchaussade De Chaumont A, Duverger V. Polysplenia syndrome. J Visc Surg. 2011; 148:e395–e396.11. Ditchfield MR, Hutson JM. Intestinal rotational abnormalities in polysplenia and asplenia syndromes. Pediatr Radiol. 1998; 28:303–306.12. Vijayakumar V, Brandt T. Prolonged survival with isolated levocardia and situs inversus. Cleve Clin J Med. 1991; 58:243–247.13. Pickhardt PJ, Bhalla S. Intestinal malrotation in adolescents and adults: spectrum of clinical and imaging features. AJR Am J Roentgenol. 2002; 179:1429–1435.14. Budhiraja S, Singh G, Miglani HP, Mitra SK. Neonatal intestinal obstruction with isolated levocardia. J Pediatr Surg. 2000; 35:1115–1116.15. Gayer G, Apter S, Jonas T, et al. Polysplenia syndrome detected in adulthood: report of eight cases and review of the literature. Abdom Imaging. 1999; 24:178–184.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Visceral heterotaxy syndrome induced by retinoids in mouse embryo
- Heterotaxy Syndrome
- Diabetes mellitus due to agenesis of the dorsal pancreas in a patient with heterotaxy syndrome
- Pancreaticoduodenectomy performed in a patient with situs ambiguous accompanied with isolated levocardia, malrotation, and normal spleen
- Isolated Adrenal Injury after Blunt Abdominal Trauma without Visceral Organ Injury
