Current Concepts in Cardiac CT Angiography for Patients With Acute Chest Pain
- Affiliations
-
- 1Department of Diagnostic Radiology, CHA Medical University Hospital, Seongnam, Korea.
- 2Department of Diagnostic Radiology, Chung-Ang University College of Medicine, Seoul, Korea.
- 3Department of Cardiology, CHA Medical University Hospital, Seongnam, Korea.
- 4Department of Diagnostic Radiology, University of Maryland, Baltimore, Maryland, USA. cwhite@umm.edu
- KMID: 1826171
- DOI: http://doi.org/10.4070/kcj.2010.40.11.543
Abstract
- This article presents specific examples of delayed diagnosis of acute coronary syndrome, acute aortic dissection, and pulmonary embolism resulting from evaluating patients with nonspecific acute chest pain who did not undergo immediate dedicated coronary CT angiography (CTA) or triple rule-out protocol (TRO). These concrete examples of delayed diagnosis may advance the concept of using cardiac CTA (i.e., dedicated coronary CTA versus TRO) to triage patients with nonspecific acute chest pain. This article also provides an overall understanding of how to choose the most appropriate examination based on the specific clinical situation in the emergency department (i.e., dedicated coronary CTA versus TRO versus dedicated pulmonary or aortic CTA), how to interpret the CTA results, and the pros and cons of biphasic versus triphasic administration of intravenous contrast material during TRO examination. A precise understanding of various cardiac CTA protocols will improve the diagnostic performance of radiologists while minimizing hazards related to radiation exposure and contrast use.
Keyword
MeSH Terms
Figure
-
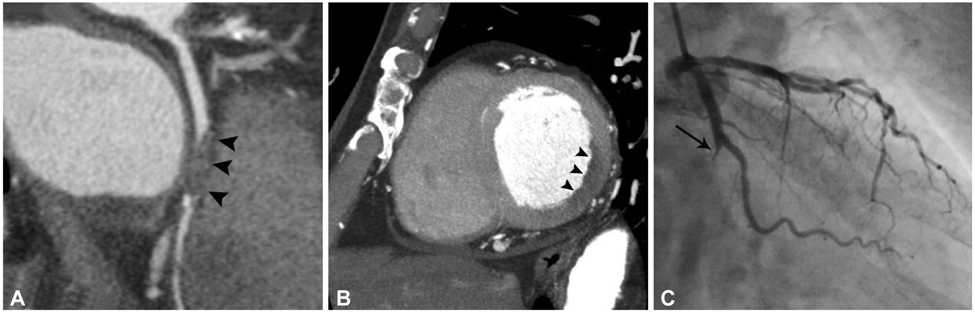
Fig. 1 Diagnostic delay in a 66-year-old male patient with acute coronary syndrome. The patient presented with acute chest pain. Dedicated coronary CT angiography was performed 7 days after symptomatic onset because the attending physician did not consider acute coronary syndrome as a primary diagnosis. A: curved multi-planar reformatted image shows total occlusion of distal left circumflex coronary artery (arrowheads). B: short axis curved multi-planar reformatted image at the basal level of the left ventricle demonstrates perfusion defect with low attenuation (arrowheads) in the territory of the left circumflex coronary artery. C: coronary angiogram shows complete obstruction (arrow) at the origin of distal left circumflex coronary artery.
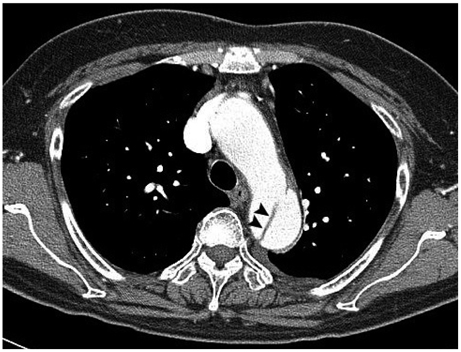
Fig. 2 Diagnostic delay in a 66-year-old female patient with Stanford type B dissection. This patient had a history of coronary stent insertion 2 years ago. The patient presented with acute chest pain to the emergency department. Emergent coronary angiography showed no significant stenosis in the coronary arteries. A Stanford type B aortic dissection (arrowheads) is noted on a trans-axial CT image at the level of aortic arch obtained 24 hours after coronary angiography.

Fig. 3 Diagnostic delay in a 62-year-old female patient with acute pulmonary embolism. This patient presented with nonspecific acute chest pain. As atypical chest pain of non-urgent cause was the initial impression, dedicated coronary CT angiography was performed 3 days later. Coronary artery assessment was negative. A: segmental pulmonary embolism (arrow) is noted in posterior segmental pulmonary artery of the right lower lobe on a trans-axial CT image at the level of left atrium. B: note that this finding is not identified on a trans-axial CT image with small field of view. This case shows the importance of using a wide field of view image when interpreting dedicated coronary CT angiography.

Fig. 4 A case of negative coronary angiography and dedicated aortic CT angiography in a 42-year-old male patient with nonspecific acute chest pain. The patient presented with severe acute chest pain in both the anterior chest and back. Emergent coronary angiography was negative. Dedicated aortic CT angiography performed on the next day was also negative. The cause of acute chest pain in the patient was determined to be esophageal spasm.
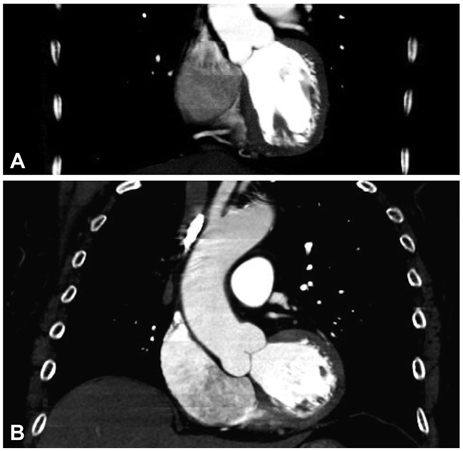
Fig. 5 Typical Z axis coverage in dedicated coronary CT angiography versus triple rule-out study. A: the field of view in a dedicated coronary CT angiography is demonstrated. B: note the increased Z axis length in the triple rule-out study compared with dedicated coronary CT angiography.
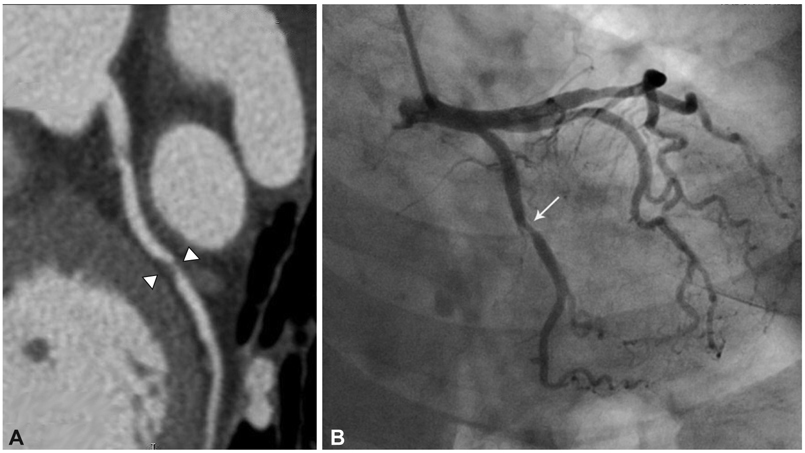
Fig. 6 A 67-year-old female patient with a critical coronary artery stenosis (>70%) in a triple rule-out study. A: critical coronary artery stenosis (>70%, arrowheads) with non-calcified plaque is identified at the proximal left circumflex coronary artery on a curved multi-planar reformatted image. B: critical coronary artery stenosis (arrow) is also identified in the same segment on coronary angiography.

Fig. 7 Mild streak artifact in a triple rule-out study using a biphasic administration of contrast material. There is no significant steak artifact in the right coronary artery (arrow), even with a high concentration of contrast material within the right ventricle.
Reference
-
1. Bastarrika G, Thilo C, Headden GF, Zwerner PL, Costello P, Schoepf UJ. Cardiac CT in the assessment of acute chest pain in the emergency department. AJR Am J Roentgenol. 2009. 193:397–409.2. Lee HY, Yoo SM, White CS. Coronary CT angiography in emergency department patients with acute chest pain: triple rule-out protocol versus dedicated coronary CT angiography. Int J Cardiovasc Imaging. 2009. 25:319–326.3. Halpern EJ. Triple rule-out CT angiography for evaluation of acute chest pain and possible acute coronary syndrome. Radiology. 2009. 252:332–345.4. Johnson TR, Nikolaou K, Wintersperger BJ, et al. Optimization of contrast material administration for electrocardiogram-gated computed tomographic angiography of the chest. J Comput Assist Tomogr. 2007. 31:265–271.5. Frauenfelder T, Appenzeller P, Karlo C, et al. Triple rule-out CT in the emergency department: protocols and spectrum of imaging findings. Eur Radiol. 2009. 19:789–799.6. Litmanovich D, Zamboni GA, Hauser TH, Lin PJ, Clouse ME, Raptopoulos V. ECG-gated chest CT angiography with 64-MDCT and triphasic IV contrast administration regimen in patients with acute nonspecific chest pain. Eur Radiol. 2008. 18:308–317.7. Shuman WP, Branch KR, May JM, et al. Whole-chest 64-MDCT of emergency department patients with nonspecific chest pain: radiation dose and coronary artery image quality with prospective ECG triggering versus retrospective ECG gating. AJR Am J Roentgenol. 2009. 192:1662–1667.8. Johnson TR, Nikolaou K, Becker A, et al. Dual-source CT for chest pain assessment. Eur Radiol. 2008. 18:773–780.9. Schertler T, Scheffel H, Frauenfelder T, et al. Dual-source computed tomography in patients with acute chest pain: feasibility and image quality. Eur Radiol. 2007. 17:3179–3188.10. Takakuwa KM, Halpern EJ. Evaluation of a "triple rule-out" coronary CT angiography protocol: use of 64-Section CT in low-to-moderate risk emergency department patients suspected of having acute coronary syndrome. Radiology. 2008. 248:438–446.11. Pozen MW, D'Agostino RB, Selker HP, Sytkowski PA, Hood WB Jr. A predictive instrument to improve coronary-care-unit admission practices in acute ischemic heart disease. A prospective multicenter clinical trial. N Engl J Med. 1984. 310:1273–1278.12. Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Rregistry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000. 283:897–903.13. Abcarian PW, Sweet JD, Watabe JT, Yoon HC. Role of a quantitative D-dimer assay in determining the need for CT angiography of acute pulmonary embolism. AJR Am J Roentgenol. 2004. 182:1377–1381.14. Klompas M. Does this patient have an acute thoracic aortic dissection? JAMA. 2002. 287:2262–2272.15. Viljanen T. Diagnostic difficulties in aortic dissection. Retrospective study of 89 surgically treated patients. Ann Chir Gynaecol. 1986. 75:328–332.16. Rogg JG, Neve JW, Huang C, et al. The triple work-up for emergency department patients with acute chest pain: how often does it occur? J Emerg Med. 2008. [Epub ahead of print].17. van Belle A, Büller HR, Huisman MV, et al. Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography. JAMA. 2006. 295:172–179.18. von Kodolitsch Y, Schwartz AG, Nienaber CA. Clinical prediction of acute aortic dissection. Arch Intern Med. 2000. 160:2977–2982.19. Gallagher MJ, Raff GL. Use of multislice CT for the evaluation of emergency room patients with chest pain: the so-called "triple rule-out". Catheter Cardiovasc Interv. 2008. 71:92–99.20. Pannu HK, Alvarez W Jr, Fishman EK. Beta-blockers for cardiac CT: a primer for the radiologist. AJR Am J Roentgenol. 2006. 186:6 Suppl 2. S341–S345.21. Hoffmann U, Bamberg F, Chae CU, et al. Coronary computed tomography angiography for early triage of patients with acute chest pain: the ROMICAT (Rule Out Myocardial Infarction using Computer Assisted Tomography) trial. J Am Coll Cardiol. 2009. 53:1642–1650.22. Hamon M, Biondi-Zoccai GC, Malagutti P, et al. Diagnostic performance of multislice spiral computed tomography of coronary arteries as compared with conventional invasive coronary angiography: a meta-analysis. J Am Coll Cardiol. 2006. 48:1896–1910.23. Dokainish H, Pillai M, Murphy SA, et al. Prognostic implications of elevated troponin in patients with suspected acute coronary syndrome but no critical epicardial coronary disease: a TACTICS-TIMI-18 substudy. J Am Coll Cardiol. 2005. 45:19–24.24. Patel MR, Chen AY, Peterson ED, et al. Prevalence, predictors, and outcomes of patients with non-ST-segment elevation myocardial infarction and insignificant coronary disease: results from the can rapid risk stratification of unstable angina patients suppress adverse outcomes with early implementation of the ACC/AHA guidelines (CRUSADE) initiative. Am Heart J. 2006. 152:641–647.25. Goldstein JA, Gallagher MJ, O'Neill WW, Ross MA, O'Neil BJ, Raff GL. A randomized controlled trial of multi-slice coronary computed tomography for evaluation of acute chest pain. J Am Coll Cardiol. 2007. 49:863–871.26. Fleischmann D, Lin M. Remy-Jardin M, Remy J, editors. Contrast medium utilization. Integrated Cardiothoracic Imaging with MDCT. 2008. Berlin, Germany: Springer;53–63.27. Jakobs TF, Becker CR, Ohnesorge B, et al. Multislice helical CT of the heart with retrospective ECG gating: reduction of radiation exposure by ECG-controlled tube current modulation. Eur Radiol. 2002. 12:1081–1086.28. Poll LW, Cohnen M, Brachten S, Ewen K, Mödder U. Dose reduction in multi-slice CT of the heart by use of ECG-controlled tube current modulation ("ECG pulsing"): phantom measurements. Rofo. 2002. 174:1500–1505.29. Husmann L, Valenta I, Gaemperli O, et al. Feasibility of low-dose coronary CT angiography: first experience with prospective ECG-gating. Eur Heart J. 2008. 29:191–197.30. Stolzmann P, Scheffel H, Schertler T, et al. Radiation dose estimates in dual-source computed tomography coronary angiography. Eur Radiol. 2008. 18:592–599.31. Scheffel H, Alkadhi H, Leschka S, et al. Low-dose CT coronary angiography in the step-and-shoot mode: diagnostic performance. Heart. 2008. 94:1132–1137.32. Hirai N, Horiguchi J, Fujioka C, et al. Prospective versus retrospective ECG-gated 64-detector coronary CT angiography: assessment of image quality, stenosis, and radiation dose. Radiology. 2008. 248:424–430.33. Ketelsen D, Luetkhoff MH, Thomas C, et al. Estimation of the radiation exposure of a chest pain protocol with ECG-gating in dual-source computed tomography. Eur Radiol. 2009. 19:37–41.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Current Concepts of Vulnerable Plaque on Coronary CT Angiography
- Normal coronary CT angiography with subsequent adverse cardiac events
- Post-Infarct Cardiac Free Wall Rupture Detected by Multi-Detector Computed Tomography
- Debates over NICE Guideline Update: What Are the Roles of Nuclear Cardiology in the Initial Evaluation of Stable Chest Pain?
- Evolution of Cardiac CT Imaging and Education in Singapore
