Three Cases of Non-Surgical Treatment of Stent Loss During Percutaneous Coronary Intervention
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea. leejongm@catholic.ac.kr
- KMID: 1826143
- DOI: http://doi.org/10.4070/kcj.2010.40.10.530
Abstract
- Percutaneous coronary intervention with stenting is widely used for ischemic heart disease. Because stent loss, which occurs rarely during the procedure, might have dire consequences, such as bleeding, stent embolism, acute myocardial infarction, emergency coronary artery bypass graft, and death, appropriate treatment is needed as soon as stent loss occurs. We report three cases of stent loss which were successfully treated with three different non-surgical methods.
MeSH Terms
Figure
-

Fig. 1 Case 1. A: left coronary angiography showed chronic total occlusion of the proximal left anterior descending artery (LAD) and severe, calcified stenosis of the proximal left circumflex artery. B: the lost stent {Taxus™ 3.0/20 mm (arrow)} is seen in the proximal LAD. C: the snare (arrow) was tightened around the stent. D: photography of the removed Taxus™ stent and snare.
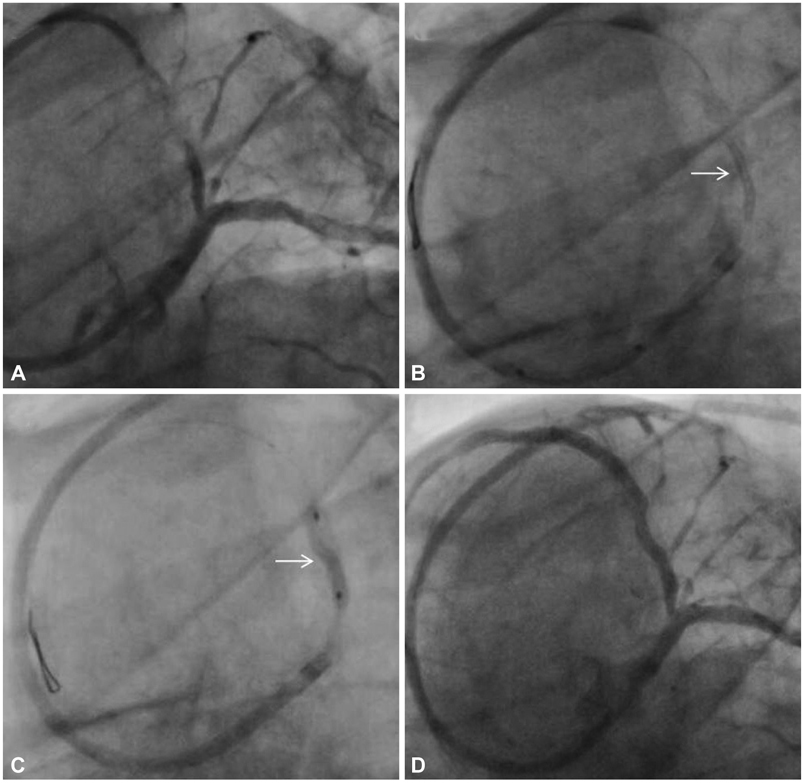
Fig. 2 Case 2. A: left coronary angiography showed severe, calcified stenosis of the proximal left anterior descending artery (LAD). B: the unexpanded lost stent {Xience V™ 3.0/15 mm stent (arrow)} is seen in the proximal LAD. C: the lost stent at the original site is depicted with an arrow; a 2.0/15 mm Ikazuchi™ balloon was placed into the stent and dilatation was performed. D: the lost stent was successfully dilated with a residual 30% stenosis.

Fig. 3 Case 3 (Initial CAG). A: left coronary angiography showed chronic total occlusion of the mid-left anterior descending artery (LAD) and 70% stenosis proximally, and 90% stenosis of the distal left circumflex artery (LCX). B-D: the unexpanded lost stent (Endeavor™ 3.0/24 mm stent, arrow) is seen in the mid-LAD. C and D: the proximal-to-distal LCX underwent stenting with a PICO™ 3.0/24 mm stent and an Endeavor™ 2.75/18 mm stent, respectively. CAG: coronary angiography.

Fig. 4 Case 3 (Follow up CAG 1 month). A: a 90% stenosis and the lost stent are apparent in the proximal LAD. B: a guide wire was passed into the lesion and stent. C: using a 3.0/15 mm Kaneka RX™ balloon dilatation was performed to 6 atm. Using an Endeavor™ 3.5/15 mm stent, the lost stent was compressed and then inserted. D: final Coronary angiography showed recovery of the hemodynamic profile. CAG: coronary angiography.
Cited by 2 articles
-
Re-mobilization of Lost Coronary Stent From the Axillary Artery to the Femoral Artery
Jeong Seok Lee, Hack-Lyoung Kim, Jae-Bin Seo, Woo-Hyun Lim, Eun Gyu Kang, Woo-Young Chung, Sang-Hyun Kim, Zoo-Hee Jo, Myung-A Kim
J Lipid Atheroscler. 2016;5(1):87-92. doi: 10.12997/jla.2016.5.1.87.Treatment of Stent Dislodgement Complicated by Coronary Artery Dissection using Parallel Wire Technique and Small Balloon
Su Young Kim, Seung-Hee Han, Kyung Han Kim, Moo Hyun Kim, Jong Sung Park
Kosin Med J. 2013;28(1):55-60. doi: 10.7180/kmj.2013.28.1.55.
Reference
-
1. Al Suwaidi J, Berger PB, Holmes DR Jr. Coronary artery stents. JAMA. 2000. 284:1828–1836.2. Park JG, Kim MH, Bae YJ, et al. Removal of dislodged stent by using 8Fr sheath and forceps during transradial coronary stenting. Korean Circ J. 2000. 30:1312–1315.3. Yang SS, Moon GH, Kim DH, et al. A case of a detached and entrapped stent balloon catheter debris after coronary stenting. Korean Circ J. 2001. 31:584–587.4. Eggebrecht H, Haude M, von Birgelen C, et al. Nonsurgical retrieval of embolized coronary stents. Catheter Cardiovasc Interv. 2000. 51:432–440.5. Brilakis ES, Best PJ, Elesber AA, et al. Incidence, retrieval methods, and outcomes of stent loss during percutaneous coronary intervention. Catheter Cardiovasc Interv. 2005. 66:333–340.6. Lohavanichbutr K, Webb JG, Carere RG, et al. Mechanisms, management, and outcome of failure of delivery of coronary stents. Am J Cardiol. 1999. 83:779–781.7. Laarman G, Muthusamy TS, Swart H, et al. Direct coronary stent implantation: safety, feasibility, and predictors of success of the strategy of direct coronary stent implantation. Catheter Cardiovasc Interv. 2001. 52:443–448.8. Holmes DR Jr, Garratt KN, Popma J. Stent complications. J Invasive Cardiol. 1998. 10:385–395.9. Hoang V, Urban V, Chatelain P, et al. Randomized evaluation of 6 French Voda-type guiding catheters for left coronary artery angioplasty. Cathet Cardiovasc Diagn. 1995. 35:53–56.10. Lee HY, Kim BH, Yoo WS, et al. Successful removal of a dislodged stent using a gooseneck snare. Korean J Med. 2008. 75:Suppl. S843–S847.11. Feldman T. Tricks for overcoming difficult stent delivery. Catheter Cardiovasc Interv. 1999. 48:285–286.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Trapped Stent in the Left Coronary Sinus in a Myocardial Infarction Patient
- Recent Advances in Percutaneous Coronary Intervention in Coronary Artery Disease
- Retrieval of a Partially Degloved Stent Strut During Percutaneous Coronary Intervention
- Percutaneous Coronary Intervention in Ischemic Heart Disease
- Perioperative management for patients undergoing noncardiac surgery after percutaneous coronary intervention
