MR Imaging of a Bilateral Lateral Segmental Anomalous Origin of the Lateral Head of the Gastrocnemius Muscles: A Case Report
- Affiliations
-
- 1Department of Radiology, Seoul Paik Hospital, Inje University College of Medicine, Seoul, Korea. jcshim96@unitel.co.kr
- KMID: 1819787
- DOI: http://doi.org/10.3348/jksr.2014.71.2.97
Abstract
- A variety of anatomic variations of the gastrocnemius muscle have been identified, predominantly through cadaver studies. Magnetic resonance imaging (MRI) findings of anomalies of the medial head of the gastrocnemius muscle have also been well reported, but anomalies of the lateral head of the gastrocnemius muscle have been less frequently reported. We present a case of an anatomic variation of the lateral head of the gastrocnemius muscle detected as an incidental finding on MRI.
MeSH Terms
Figure
-
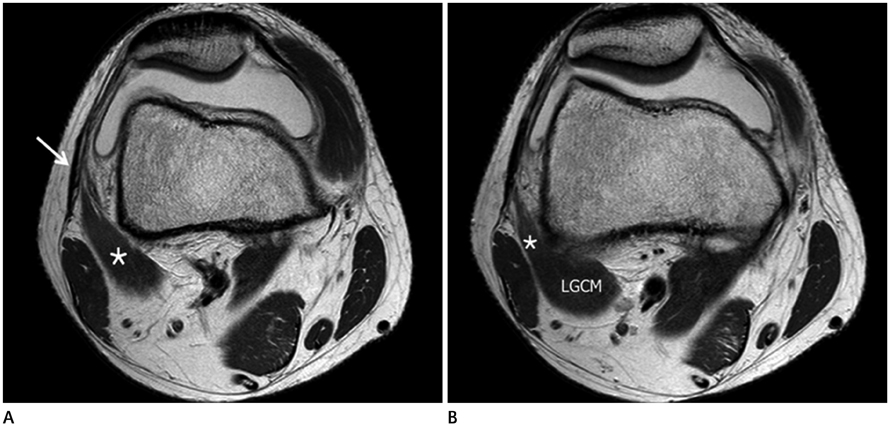
Fig. 1 Axial MR images of the right knee. A. Right knee shows an anomalous muscle (asterisk) which originates from the iliotibial band (arrow). B. Inferiorly, this muscle (asterisk) combines with the body of the lateral head of gastrocnemius muscle (LGCM), which normally originates from the lateral condyle of the femur.

Fig. 2 Axial and coronal MR images of the left knee. A. Axial scan shows an anomalous muscle (asterisk) originating from the iliotibial band (arrow). This muscle also merges with the body of the lateral head of gastrocnemius muscle (LGCM), as is also the case in the right knee (not shown). B. Serial coronal scans from posterior to anterior confirm the body of the LGCM normally originating from the posterior aspect of the lateral femoral condyle, and the lateral segment of the muscle (asterisk) originating from the iliotibial band (arrow). Osteoarthrosis with lateral femoral condylar grade 2 cartilage lesions are also noted.
Reference
-
1. Bergman RA, Afifi AK, Miyauchi R. Gastrocnemius and soleus. Illustrated encyclopedia of human anatomic variation. Updated February 12, 2013. Accessed May 31, 2013. Available from http://www.anatomyatlases.org/.2. Arce YV, Almirón YP, Daz MAR, Nuñez CGE. Anatomic variations of the gastrocnemius muscle. Braz J Morphol Sci. 2008; 25:157–214.3. Singla RK, Gupta R. Caput tertium Gastrocnemius: a case report. J Clin Diagn Res. 2012; 6:1059–1061.4. Elias DA, White LM, Rubenstein JD, Christakis M, Merchant N. Clinical evaluation and MR imaging features of popliteal artery entrapment and cystic adventitial disease. AJR Am J Roentgenol. 2003; 180:627–632.5. Kim HK, Shin MJ, Kim SM, Lee SH, Hong HJ. Popliteal artery entrapment syndrome: morphological classification utilizing MR imaging. Skeletal Radiol. 2006; 35:648–658.6. Yu JS, Resnick D. MR imaging of the accessory soleus muscle appearance in six patients and a review of the literature. Skeletal Radiol. 1994; 23:525–528.7. Assoun J, Railhac JJ, Richardi G, Fajadet P, Fourcade D, Sans N. CT and MR of accessory soleus muscle. J Comput Assist Tomogr. 1995; 19:333–335.8. Cheung Y, Rosenberg ZS. MR imaging of the accessory muscles around the ankle. Magn Reson Imaging Clin N Am. 2001; 9:465–473. x9. Duc SR, Wentz KU, Käch KP, Zollikofer CL. First report of an accessory popliteal muscle: detection with MRI. Skeletal Radiol. 2004; 33:429–431.10. Kim HK, Laor T, Racadio JM. MR imaging assessment of the lateral head of the gastrocnemius muscle: prevalence of segmental anomalous origins in children and young adults. Pediatr Radiol. 2008; 38:1300–1305.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Tendon Reflex Responses between Two Heads of Gastrocnemius in Spastic Hemiplegia and Healthy Subjects
- The Co-existence of the Gastrocnemius Tertius and Accessory Soleus Muscles
- Bilateral Fractured of the Fabella
- Popliteal Artery Entrapment Syndrome caused by a Anomalous Origin of the Gastrocnemius Muscle: Case Report
- Surface Mapping of Motor Points of Gastrocnemius and Soleus Muscles
