Outcomes and Prognostic Factors of Endovascular Abdominal Aortic Aneurysm Repair in Patients with Hostile Neck Anatomy
- Affiliations
-
- 1Department of Radiology, Chonnam National University Hospital, Gwangju, Korea. kjkrad@chonnam.ac.kr
- 2Department of Vascular Surgery, Chonnam National University Hospital, Gwangju, Korea.
- 3Department of Radiology, St. Carollo Hospital, Suncheon, Korea.
- 4Department of Radiology, Donggunsan Hospital, Gunsan, Korea.
- KMID: 1819747
- DOI: http://doi.org/10.3348/jksr.2012.67.5.323
Abstract
- PURPOSE
To evaluate the outcomes and find the prognostic factors of endovascular abdominal aortic aneurysm repair (EVAR) in patients with hostile neck anatomy of the abdominal aorta.
MATERIALS AND METHODS
This study was performed on 100 patients with abdominal aneurysm who were treated with EVAR between March 2006 and December 2010. We divided the patients into two groups: good neck anatomy (GNA), and hostile neck anatomy (HNA) and then compared the primary success rate and the incidence rate of complications with EVAR between the two groups. Our aim was to determine the factors related to the complications of EVAR among HNA types.
RESULTS
There were no significant differences of primary success rate and incidence rate of complications between the two groups. Among the types of HNA, the short neck angle [odd ratio (OR), 4.23; 95% confidence interval (CI), 1.21-18.70; p = 0.023] and large neck angle (OR, 2.58; 95% CI, 0.15-11.85; p = 0.031) showed a low primary success rate. The short neck angle (OR, 2.32; 95% CI, 1.18-12.29; p = 0.002) and large neck angle (OR, 4.67; 95% CI, 0.14-19.07; p = 0.032) showed a high incidence rate of early type 1 complication. In the case of the large neck angle (OR, 3.78; 95% CI, 0.96-20.80; p = 0.047), the large neck thrombus (OR, 2.23; 95% CI, 0.24-7.12; p = 0.035) and large neck calcification (OR, 2.50; 95% CI, 0.08-18.37; p = 0.043) showed a high incidence rate of complications within a year.
CONCLUSION
The results suggest that patients with hostile neck anatomy can be treated with EVAR successfully, although there was a higher incidence of complications in patients with a short neck length, severe neck angulation, circumferential thrombosis, and calcified proximal neck.
Figure
-
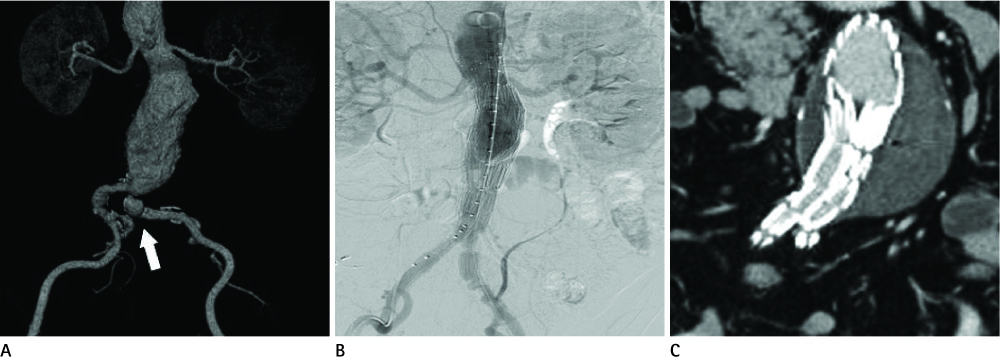
Fig. 1 No hostile neck features, a 59-year-old man. A. Volume rendering image shows infrarenal abdominal aortic aneurysm (sac diameter: 42 mm) with aneurysmal dilatation of left common iliac artery (arrow). There is no adverse feature in the proximal aortic neck. B. Completion angiogram shows successful deployment of Zenith® 32-118-12 mm. C. Three months after EVAR, there was no complication on follow up CT image. Note.-EVAR = endovascular abdominal aortic aneurysm repair
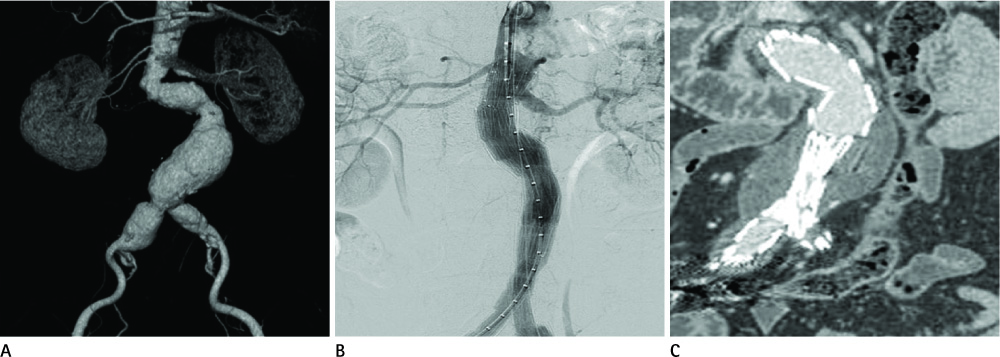
Fig. 2 One hostile neck feature, an 84-year-old man. A. Volume rendering image shows infrarenal abdominal aortic aneurysm (sac diameter: 46 mm) with aneurysmal dilatation of both common iliac arteries. Neck angulation is 84°. B. Completion angiogram shows no immediate complication after deployment of Zenith® 28-133-12 mm. C. Six months after EVAR, there was no complication on follow up abdomen CTA. Note.-CTA = CT angiography, EVAR = endovascular abdominal aortic aneurysm repair

Fig. 3 Two hostile neck features, an 85-year-old man. A. Volume rendering image shows infrarenal abdominal aortic aneurysm (sac diameter: 48 mm) with calcified proximal neck and conical neck. B. Follow up angiogram shows Type Ia endoleak (arrow) after deployment of Zenith® 30-155 mm. C. After deployment of aortic ring (14-90 mm), type Ia endoleak was improved. D. After 1 month, there was no complication on follow up abdomen CTA. Note.-CTA = CT angiography
Reference
-
1. Rimon U, Garniek A, Golan G, Bensaid P, Galili Y, Schneiderman J, et al. Resolved abdominal aortic aneurysms following stent graft treatment: a report of five cases. Cardiovasc Intervent Radiol. 2004. 27:143–147.2. Ouriel K, Tanquilut E, Greenberg RK, Walker E. Aortoiliac morphologic correlations in aneurysms undergoing endovascular repair. J Vasc Surg. 2003. 38:323–328.3. Arko FR, Filis KA, Seidel SA, Gonzalez J, Lengle SJ, Webb R, et al. How many patients with infrarenal aneurysms are candidates for endovascular repair? The Northern California experience. J Endovasc Ther. 2004. 11:33–40.4. Harris PL, Vallabhaneni SR, Desgranges P, Becquemin JP, van Marrewijk C, Laheij RJ. Incidence and risk factors of late rupture, conversion, and death after endovascular repair of infrarenal aortic aneurysms: the EUROSTAR experience. European Collaborators on Stent/graft techniques for aortic aneurysm repair. J Vasc Surg. 2000. 32:739–749.5. Hovsepian DM, Hein AN, Pilgram TK, Cohen DT, Kim HS, Sanchez LA, et al. Endovascular abdominal aortic aneurysm repair in 144 patients: correlation of aneurysm size, proximal aortic neck length, and procedure-related complications. J Vasc Interv Radiol. 2001. 12:1373–1382.6. Mohan IV, Laheij RJ, Harris PL. EUROSTAR COLLABORATORS. Risk factors for endoleak and the evidence for stent-graft oversizing in patients undergoing endovascular aneurysm repair. Eur J Vasc Endovasc Surg. 2001. 21:344–349.7. Stanley BM, Semmens JB, Mai Q, Goodman MA, Hartley DE, Wilkinson C, et al. Evaluation of patient selection guidelines for endoluminal AAA repair with the Zenith Stent-Graft: the Australasian experience. J Endovasc Ther. 2001. 8:457–464.8. Sternbergh WC 3rd, Carter G, York JW, Yoselevitz M, Money SR. Aortic neck angulation predicts adverse outcome with endovascular abdominal aortic aneurysm repair. J Vasc Surg. 2002. 35:482–486.9. Zarins CK, Bloch DA, Crabtree T, Matsumoto AH, White RA, Fogarty TJ. Stent graft migration after endovascular aneurysm repair: importance of proximal fixation. J Vasc Surg. 2003. 38:1264–1272. discussion 1272.10. Dias NV, Resch T, Malina M, Lindblad B, Ivancev K. Intraoperative proximal endoleaks during AAA stent-graft repair: evaluation of risk factors and treatment with Palmaz stents. J Endovasc Ther. 2001. 8:268–273.11. Dillavou ED, Muluk SC, Rhee RY, Tzeng E, Woody JD, Gupta N, et al. Does hostile neck anatomy preclude successful endovascular aortic aneurysm repair? J Vasc Surg. 2003. 38:657–663.12. Aburahma AF, Campbell JE, Mousa AY, Hass SM, Stone PA, Jain A, et al. Clinical outcomes for hostile versus favorable aortic neck anatomy in endovascular aortic aneurysm repair using modular devices. J Vasc Surg. 2011. 54:13–21.13. Gitlitz DB, Ramaswami G, Kaplan D, Hollier LH, Marin ML. Endovascular stent grafting in the presence of aortic neck filling defects: early clinical experience. J Vasc Surg. 2001. 33:340–344.14. Choke E, Munneke G, Morgan R, Belli AM, Loftus I, McFarland R, et al. Outcomes of endovascular abdominal aortic aneurysm repair in patients with hostile neck anatomy. Cardiovasc Intervent Radiol. 2006. 29:975–980.15. Greenberg R, Fairman R, Srivastava S, Criado F, Green R. Endovascular grafting in patients with short proximal necks: an analysis of short-term results. Cardiovasc Surg. 2000. 8:350–354.16. Robbins M, Kritpracha B, Beebe HG, Criado FJ, Daoud Y, Comerota AJ. Suprarenal endograft fixation avoids adverse outcomes associated with aortic neck angulation. Ann Vasc Surg. 2005. 19:172–177.17. Cao P, Verzini F, Parlani G, Rango PD, Parente B, Giordano G, et al. Predictive factors and clinical consequences of proximal aortic neck dilatation in 230 patients undergoing abdominal aorta aneurysm repair with self-expandable stent-grafts. J Vasc Surg. 2003. 37:1200–1205.18. Fairman RM, Velazquez OC, Carpenter JP, Woo E, Baum RA, Golden MA, et al. Midterm pivotal trial results of the Talent Low Profile System for repair of abdominal aortic aneurysm: analysis of complicated versus uncomplicated aortic necks. J Vasc Surg. 2004. 40:1074–1082.19. Albertini JN, Perdikides T, Soong CV, Hinchliffe RJ, Trojanowska M, Yusuf SW. Endovascular repair of abdominal aortic aneurysms in patients with severe angulation of the proximal neck using a flexible stent-graft: European Multicenter Experience. J Cardiovasc Surg (Torino). 2006. 47:245–250.20. Buth J, van Marrewijk CJ, Harris PL, Hop WC, Riambau V, Laheij RJ. EUROSTAR Collaborators. Outcome of endovascular abdominal aortic aneurysm repair in patients with conditions considered unfit for an open procedure: a report on the EUROSTAR experience. J Vasc Surg. 2002. 35:211–221.21. Hobo R, Sybrandy JE, Harris PL, Buth J. EUROSTAR Collaborators. Endovascular repair of abdominal aortic aneurysms with concomitant common iliac artery aneurysm: outcome analysis of the EUROSTAR Experience. J Endovasc Ther. 2008. 15:12–22.22. May J, White GH, Ly CN, Jones MA, Harris JP. Endoluminal repair of abdominal aortic aneurysm prevents enlargement of the proximal neck: a 9-year life-table and 5-year longitudinal study. J Vasc Surg. 2003. 37:86–90.23. Leurs LJ, Buth J, Harris PL, Blankensteijn JD. Impact of study design on outcome after endovascular abdominal aortic aneurysm repair. A comparison between the randomized controlled DREAM-trial and the observational EUROSTAR-registry. Eur J Vasc Endovasc Surg. 2007. 33:172–176.24. Waasdorp EJ, de Vries JP, Hobo R, Leurs LJ, Buth J, Moll FL. EUROSTAR Collaborators. Aneurysm diameter and proximal aortic neck diameter influence clinical outcome of endovascular abdominal aortic repair: a 4-year EUROSTAR experience. Ann Vasc Surg. 2005. 19:755–761.25. AbuRahma AF, Campbell J, Stone PA, Nanjundappa A, Jain A, Dean LS, et al. The correlation of aortic neck length to early and late outcomes in endovascular aneurysm repair patients. J Vasc Surg. 2009. 50:738–748.26. Hobo R, Kievit J, Leurs LJ, Buth J. EUROSTAR Collaborators. Influence of severe infrarenal aortic neck angulation on complications at the proximal neck following endovascular AAA repair: a EUROSTAR study. J Endovasc Ther. 2007. 14:1–11.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Adjunctive Procedures for Challenging Endovascular Abdominal Aortic Repair: When Needed and How Effective?
- The Influence of Unfavorable Aortoiliac Anatomy on Short-Term Outcomes after Endovascular Aortic Repair
- Endovascular Repair of a Juxtarenal Abdominal Aortic Aneurysm Using a Chimney Graft
- Abdominal Aortic Aneurysm
- Thrombotic Occlusion of Stent Graft Limbs due to Severe Angulation of Aortic Neck in Endovascular Repair of Abdominal Aortic Aneurysm
