Cancer Res Treat.
2012 Dec;44(4):271-274.
Poorly Differentiated Neuroendocrine Carcinoma in a Perigastric Lymph Node from an Unknown Primary Site
- Affiliations
-
- 1Department of Internal Medicine, Chungbuk National University College of Medicine, Cheongju, Korea. hyesukhan@chungbuk.ac.kr
- 2Department of Pathology, Chungbuk National University College of Medicine, Cheongju, Korea.
- 3Department of Surgery, Chungbuk National University College of Medicine, Cheongju, Korea.
Abstract
- Neuroendocrine carcinomas from an unknown primary site are uncommon. The authors report on a case of neuroendocrine carcinoma in a perigastric lymph node (LN) with no primary site. A 52-year-old male patient with early gastric adenocarcinoma underwent treatment by endoscopic submucosal dissection, and, six months later, findings on a computed tomographic scan of the abdomen revealed a LN enlargement measuring 2.0 cm in the perigastric region. The patient underwent subtotal gastrectomy and regional LN dissection under a suggestive preoperative diagnosis of gastric adenocarcinoma with LN metastasis. However, microscopically, no residual tumor was found in the stomach, and the perigastric LN showed poorly differentiated neuroendocrine carcinoma (PDNEC). After an extensive workup, no primary site was identified. The patient also received four cycles of etoposide and cisplatin. Despite its extremely rare incidence, this case suggests that PDNEC of an unknown primary site is limited to a single site, and that resection should be considered in combination with chemotherapy.
MeSH Terms
Figure
-
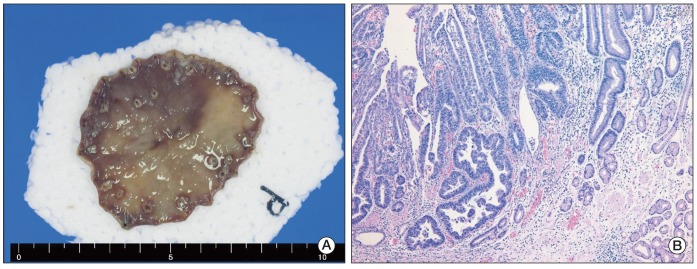
Fig. 1 (A) Resected specimen of type IIc early gastric cancer obtained by endoscopic submucosal dissection. (B) Histologic examination revealed well differentiated adenocarcinoma restricted to the mucosa without lymphovascular invasion or perineural invasion (H&E staining, ×100).
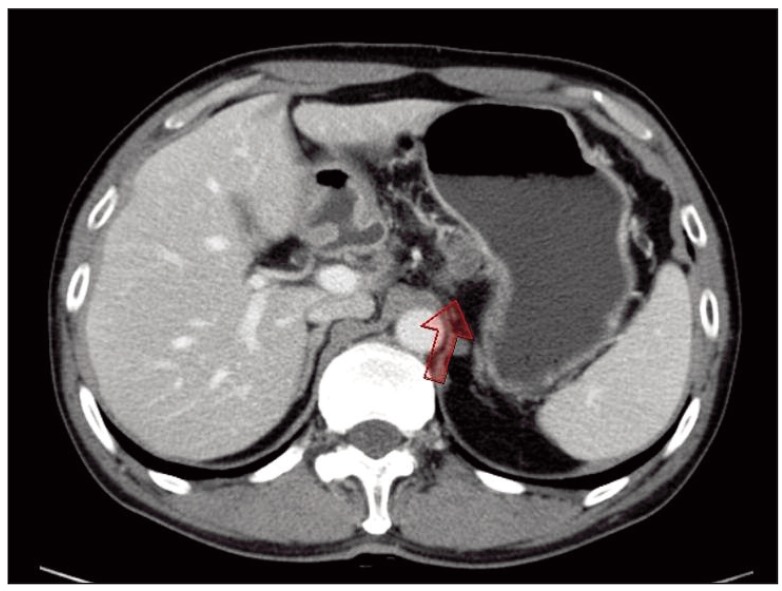
Fig. 2 Computed tomograph of the abdomen showing lymph node enlargement in the perigastric area.
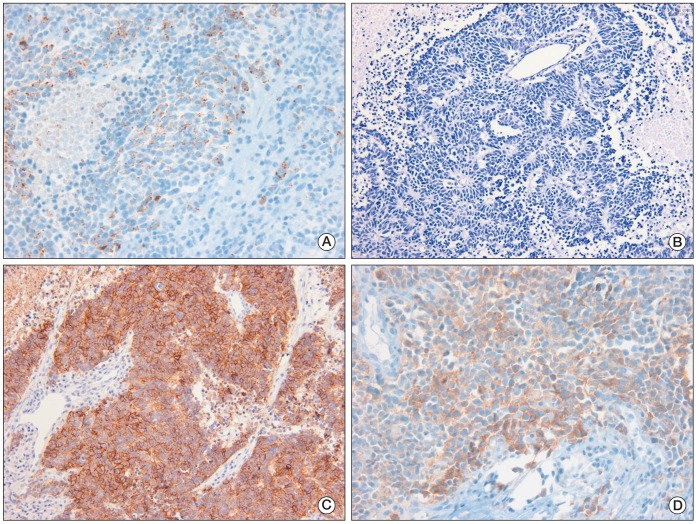
Fig. 3 Microscopic examination of the perigastric lymph node showing that the tumor was composed of monotonous round cells with scant eosinophilic cytoplasm (A, H&E staining, ×200). Tumor cells were positive for CD56 (B, ×100), synaptophysin A (C, ×200), and chromogranin (D, ×200).
Reference
-
1. Hainsworth JD, Johnson DH, Greco FA. Poorly differentiated neuroendocrine carcinoma of unknown primary site: a newly recognized clinicopathologic entity. Ann Intern Med. 1988; 109:364–371. PMID: 2841895.2. Spigel DR, Hainsworth JD, Greco FA. Neuroendocrine carcinoma of unknown primary site. Semin Oncol. 2009; 36:52–59. PMID: 19179188.
Article3. Bajetta E, Catena L, Procopio G, Bichisao E, Ferrari L, Della Torre S, et al. Is the new WHO classification of neuroendocrine tumours useful for selecting an appropriate treatment? Ann Oncol. 2005; 16:1374–1380. PMID: 15939719.
Article4. Hainsworth JD, Spigel DR, Litchy S, Greco FA. Phase II trial of paclitaxel, carboplatin, and etoposide in advanced poorly differentiated neuroendocrine carcinoma: a Minnie Pearl Cancer Research Network Study. J Clin Oncol. 2006; 24:3548–3554. PMID: 16877720.
Article5. Boghossian V, Owen ID, Nuli B, Xiao PQ. Neuroendocrine (Merkel cell) carcinoma of the retroperitoneum with no identifiable primary site. World J Surg Oncol. 2007; 5:117. PMID: 17949500.
Article6. Hisamori S, Okabe H, Yoshizawa A, Sakai Y. A case of long-term recurrence-free poorly differentiated neuroendocrine carcinoma of lymph nodes treated by surgical resection without any chemotherapy. Int J Clin Oncol. 2010; 15:493–496. PMID: 20224882.
Article7. Kuwabara H, Mori H, Uda H, Takei K, Ishibashi Y, Takatani N. Nodal neuroendocrine (Merkel cell) carcinoma without an identifiable primary tumor. Acta Cytol. 2003; 47:515–517. PMID: 12789943.8. Ueda J, Aimoto T, Nakamura Y, Hiroi M, Yamahatsu K, Hayakawa T, et al. Pancreaticoduodenal lymph node metastasis of neuroendocrine carcinoma of unknown primary associated with duodenal carcinoma. Nihon Shokakibyo Gakkai Zasshi. 2010; 107:1941–1946. PMID: 21139363.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Synchronous Gastric Adenocarcinoma and Perigastric Lymph Node Metastatic Squamous Cell Carcinoma with Unknown Primary: A Case Report
- Neuroendocrine Tumor of Unknown Primary Accompanied with Stomach Adenocarcinoma
- Metastatic Large Cell Neuroendocrine Carcinoma Combined with Gastric Adenocarcinoma
- Moderately Differentiated Neuroendocrine Carcinoma of the Larynx
- Gastric Adenocarcinoma with Coexistent Hepatoid Adenocarcinoma and Neuroendocrine Carcinoma: A Case Report
