Natural Course and Treatment Strategy of Gallbladder Polyp
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. bang7028@yuhs.ac
- KMID: 1792749
- DOI: http://doi.org/10.4166/kjg.2009.53.6.336
Abstract
- The polypoid lesions of gallbladder have explosively increased with enhanced feasibility of transabdominal ultrasonography. Most of small polyps less than 10 mm are benign and remain static for a long period. In small polyps, three to six month intervaled ultrasonography is warranted in the initial follow-up, but the duration of follow-up period is not clarified. The polypoid lesions larger than 10 mm show a quite different feature. They showed a remarkable risk of malignancy (34-88%) and should be treated by surgery. Furthermore, age more than 50 years and combined gallstone are important factors predicting malignancy in polypoid lesions of gallbladder. In addition, other factors including solitary polyp and the presence of symptoms are considered as risk factors. Laparoscopic cholecystectomy is a golden standard therapy for these polyps unless the suspicion of malignancy is high. The gallbladder polyps remain a problem of concern to both doctors and patient with the worry of malignancy. Thus, the comprehensive understanding of natural coruse of gallbladder polyp and risk factors of malignancy should be kept in mind.
MeSH Terms
Figure
-
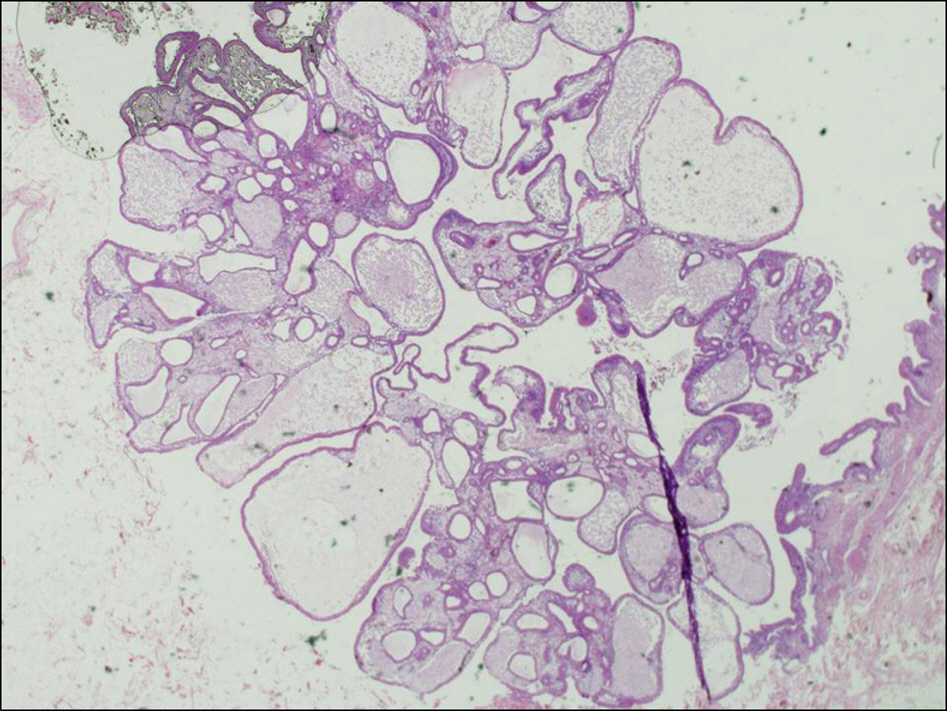
Fig. 1. Microscopic feature of cholesterol polyp. Lipid laden macrophage containing polyp was observed (H&E staining, ×100).

Fig. 2. Microscopic feature of the adenomatous polyp. The polyp composed of glandular structure with tall columnar epithelium and fibrous stroma. In the center, dilated gland and vessels sur-rounded by loose connective tissue was noted (H&E staining, ×40).

Fig. 3. Treatment algorithm of gallbladder polyps.
Cited by 4 articles
-
Recent Updates on Diagnosis, Treatment, and Follow-up of Gallbladder Polyps
Sung Ill Jang, Jae Hee Cho, Dong Ki Lee
Korean J Gastroenterol. 2020;76(3):102-107. doi: 10.4166/kjg.2020.76.3.102.Risk Factors of Gallbladder Polyp
Woo Hyun Paik
Korean J Gastroenterol. 2015;66(5):249-250. doi: 10.4166/kjg.2015.66.5.249.Analysis of gallbladder polypoid lesion size as an indication of the risk of gallbladder cancer
Ji Eun Sung, Chang Woo Nam, Yang Won Nah, Byung Sung Kim
Korean J Hepatobiliary Pancreat Surg. 2014;18(1):9-13. doi: 10.14701/kjhbps.2014.18.1.9.Preoperative predictive factors for gallbladder cholesterol polyp diagnosed after laparoscopic cholecystectomy for polypoid lesions of gallbladder
Hyojin Lee, Kihwan Kim, Inseok Park, Hyunjin Cho, Geumhee Gwak, Keunho Yang, Byung-Noe Bae, Hong-Ju Kim, Young Duk Kim
Ann Hepatobiliary Pancreat Surg. 2016;20(4):180-186. doi: 10.14701/ahbps.2016.20.4.180.
Reference
-
1. Ministry of Health and Welfare. Annual Report of the Korea Central Cancer Registry (2005 cancer incidence, 1993-2005 cancer survival). 2008.2. Christensen AH, Ishak KG. Benign tumors and pseudotumors of the gallbladder. Report of 180 cases. Arch Pathol. 1970; 90:423–432.3. Weedon D. Benign mucosal polyps. Mosby, Pathology of the gallbladder. New York: Mason;1984. p. 195.4. Yang HL, Sun YG, Wang Z. Polypod lesions of the gallbladder: diagnosis and indications for surgery. Br J Surg. 1992; 79:227–229.5. Kozuka S, Tsubone N, Yasui A, Hachisuka K. Relation of adenoma to carcinoma in the gallbladder. Cancer. 1982; 50:2226–2234.
Article6. Persley KM. Acalculous cholcystitis, cholesterolosis, adeno-myomatosis, and polyps of the gallbladder. Feldman M, Friedman LS, Brandt LJ, editors. eds.Gastrointestinal and liver disease. Volume 1. 8th ed.Philadelphia: Elsevier;2006. p. 1443–1459.7. Feldman M, Feldman M Jr. Cholesterolosis of the gallbladder: an autopsy study of 165 cases. Gastroenterology. 1954; 27:641.8. Roa I, de Aretxabala X, Araya JC, Roa J. Preneoplasitc lesions in gallbladder cancer. J Surg Oncol. 2006; 93:615–623.9. Terzi C, Sokmen S, Seckin S, Albayrak L, Ugurlu M. Polypoid lesions of the gallbladder: report of 100 cases with special reference to operative indications. Surgery. 2000; 27:622–627.
Article10. Park JY, Hong SP, Kim YJ, et al. Longterm follow up of gallbladder polyps. J Gastroenterol Hepatol. 2009; 24:219–222.
Article11. Lee KF, Wong J, Li JC, Lai PB. Polypoid lesions of the gallbladder. Am J Surg. 2004; 188:186–190.
Article12. Tsuchiya Y. Early carcinoma of the gallbladder: macroscopic features and US findings. Radiology. 1991; 179:171–175.
Article13. Aldridge MC, Bismuth H. Gallbladder cancer: the polyp-cancer sequence. Br J Surg. 1990; 77:393–394.
Article14. Eelkema HH, Hodgeson JR, Stauffer MH. Fifteen-year follow-up of polypoid lesions of gallbladder diagnosed by cholecystography. Gastroenterology. 1962; 39:144–147.15. Moriguchi H, Tazawa J, Hayashi Y, et al. Natural history of polypoid lesions in the gallbladder. Gut. 1996; 39:860–862.16. Albores-Saaverdra J, Vardaman CJ, Vuitch F. Non-neoplastic polypoid lesions and adenomas of the gallbladder. Pathol Annu. 1993; 28:145–177.17. Kubota K, Bandai Y, Noie T, et al. How should polypoid lesions of the gallbladder be treated in the era of laparoscopic cholecystectomy? Surgery. 1995; 117:481–487.
Article18. Yeh CN, Jan YY, Chao TC, Chen MF. Laparoscopic cholecystectomy for polypoid lesions of the gallbladder: a clin-icopathologic study. Surg Laparosc Endosc Percutan Tech. 2001; 11:176–181.19. Csendes A, Burgos AM, Csendes P, et al. Late follow-up of polypoid lesions of the gallbladder smaller than 10 mm. Ann Surg. 2001; 234:657–660.
Article20. Choi WB, Lee SK, Kim MH, et al. A new strategy to predict the neoplastic polyps of the gallbladder based on a scoring system using EUS. Gastrointest Endosc. 2000; 52:372–379.
Article21. Sadamato Y, Oda S, Tanaka M, et al. A useful approach to the differential diagnosis of small polypoid lesions of the gallbladder, utilizing an endoscopic ultrasound scoring system. Endoscopy. 2002; 34:959–965.
Article22. Cho JH, Park JY, Kim YJ, et al. Hypoechoic foci on EUS are simple and strong predictive factors for neoplastic gallbladder polyps. Gastrointest Endosc. 2009; 69:1244–1250.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment Guidelines for Gallbladder Polyps
- A Surgical Consideration on Gallbladder Polyp - A Proposal of Therapeutic Guideline for Gallbladder Polyp -
- Polypoid Lesions of the Gallbladder; Report of 111 Cases with Surgical Reference to Operative Indication
- Cholelithiasis as a Risk Factor for Gallbladder Cancer
- A Case of Gall Bladder Polyp in Children
