Korean J Ophthalmol.
2014 Apr;28(2):186-188. 10.3341/kjo.2014.28.2.186.
Bilateral Acute Anterior Uveitis and Optic Disc Edema Following a Snake Bite
- Affiliations
-
- 1Department of Ophthalmology, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, India. smilefriend84@yahoo.com
- KMID: 1792115
- DOI: http://doi.org/10.3341/kjo.2014.28.2.186
Abstract
- The authors wish to report a case of bilateral acute anterior uveitis and optic disc edema following a hemotoxic snake bite, in order to highlight the concomitant occurrence of these conditions and the potential adverse effects of anti-snake venom (ASV). A 35-year-old male was bitten by a viper at seventeen thirty hours, and was started on ASV. Two days following treatment he experienced sudden onset redness and painful diminution of vision in both eyes (OU). On examination, the patient's visual acuity (VA) in OU was 20/200. Examination revealed fresh keratic precipitates, cells, and flare in the anterior chamber (AC), posterior synechiae, sluggish and ill-sustained pupillary reaction, and hyperemic, edematous disc with blurred margins in OU. He was started on topical steroids, cycloplegics and intravenous methylprednisolone. Following treatment, the patient showed improvement and was continued on topical medications and oral prednisolone tapered over 3 weeks, after which VA OU improved, the AC showed no cells and flare and disc edema resolved. Uveitis and optic disc edema in snake bite can either be due to the direct toxic effects of the venom or the effect of ASV. Steroids have a beneficial role in the management of these symptoms.
Keyword
MeSH Terms
-
Acute Disease
Adult
Antivenins/*adverse effects
Glucocorticoids/administration & dosage
Humans
Hyperemia/drug therapy/etiology/pathology
Male
Methylprednisolone/administration & dosage
Papilledema/drug therapy/*etiology/pathology
Snake Bites/*complications/*therapy
Uveitis, Anterior/drug therapy/*etiology/pathology
Antivenins
Glucocorticoids
Methylprednisolone
Figure
-

Fig. 1 (A) Slit lamp photograph of the right eye showing posterior synechiae at the 3 o'clock position. (B) Slit lamp photograph of the left eye showing posterior synechiae at the 11 o'clock position.
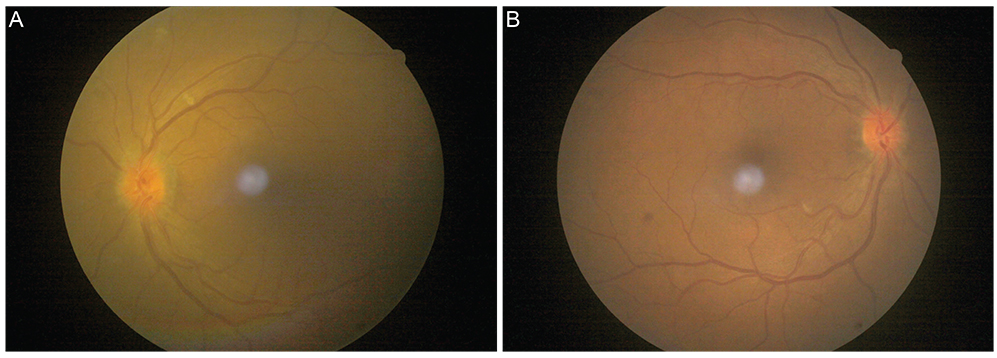
Fig. 2 Fundus photographs of the left (A) and right eye (B) showing hyperemia and blurred margins, with edema of the optic nerve head.
Reference
-
1. Nigam P, Tandon VK, Kumar R, et al. Snake bite: a clinical study. Indian J Med Sci. 1973; 27:697–704.2. Chopra PC. Optic neuritis after cobra bite. Indian Med Gaz. 1939; 74:420.3. Davenport RC, Budden FH. Loss of sight following snake bite. Br J Ophthalmol. 1953; 37:119–121.4. Mathur SP. Allergy to antivenine serum. Br J Ophthalmol. 1959; 43:50–51.5. Rao KV. Optic neuritis and ophthalmoplegia caused by snake bite. Indian J Ophthalmol. 1981; 29:243–245.6. Sanghavi NG, Amin SK, Naik RS. Bilateral optic neuritis following snake bite: a case report. J Assoc Physicians India. 1982; 30:117–118.7. Menon V, Tandon R, Sharma T, Gupta A. Optic neuritis following snake bite. Indian J Ophthalmol. 1997; 45:236–237.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Optic Disc Neovascularization in Chronic Anterior Uveitis
- Ocular Manifestations of Venomous Snake Bite over a One-year Period in a Tertiary Care Hospital
- Comparison of Optic Disc Appearance in Anterior ischemic optic neuropathy and Optic neuritis
- A Case Report of Snake bites During Pregnancy
- Association of Optic Disc Hyperfluorescence with Subclinical Macular and Optic Disc Edema in Uveitis Patients
