The Clinical Association of the Blood Pressure Variability with the Target Organ Damage in Hypertensive Patients with Chronic Kidney Disease
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea. imsejoong@hanmail.net
- 2Department of Internal Medicine, National Medical Center, Seoul, Korea.
- 3Medical Research Collaborating Center of Seoul National University Bundang Hospital, Seongnam, Korea.
- 4Department of Internal Medicine, The Catholic University of Korea College of Medicine, Uijeongbu, Korea.
- 5Department of Internal Medicine, Ewha Womans University College of Medicine, Seoul, Korea.
- 6Department of Internal Medicine, Hallym University College of Medicine, Seoul, Korea.
- 7Department of Internal Medicine, Inje University College of Medicine, Ilsan, Korea.
- 8Department of Internal Medicine, Soon Chun Hyang University College of Medicine, Cheonan, Korea.
- 9Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea.
- 10Kidney Research Institute, Seoul National University Medical Research Center, Seoul, Korea.
- KMID: 1789955
- DOI: http://doi.org/10.3346/jkms.2014.29.7.957
Abstract
- It is known that blood pressure variability (BPV) can independently affect target organ damage (TOD), even with normal blood pressure. There have been few studieson chronic kidney disease (CKD) patients. We evaluated the relationship between BPV and TOD in a cross-sectional, multicenter study on hypertensive CKD patients. We evaluated 1,173 patients using 24-hr ambulatory blood pressure monitoring. BPV was defined as the average real variability, with a mean value of the absolute differences between consecutive readings of systolic blood pressure. TOD was defined as left ventricular hypertrophy (LVH) (by the Romhilt-Estes score > or =4 in electrocardiography) and kidney injury (as determined from an estimated glomerular filtration rate [eGFR]<30 mL/min/1.73 m2 and proteinuria).The mean BPV of the subjects was 15.9+/-4.63 mmHg. BPV displayed a positive relationship with LVH in a univariate analysis and after adjustment for multi-variables (odds ratio per 1 mmHg increase in BPV: 1.053, P=0.006). In contrast, BPV had no relationship with kidney injury. These data suggest that BPV may be positively associated with LVH in hypertensive CKD patients.
Keyword
MeSH Terms
-
Adult
Aged
Blood Pressure/*physiology
Blood Pressure Monitoring, Ambulatory
Cross-Sectional Studies
Electrocardiography
Female
Glomerular Filtration Rate
Humans
Hypertension/*complications/*diagnosis
Hypertrophy, Left Ventricular/*physiopathology
Kidney/injuries
Male
Middle Aged
Odds Ratio
Proteinuria/complications
Renal Insufficiency, Chronic/*complications/*diagnosis
Figure
-

Fig. 1 Odds ratio for left ventricular hypertrophy (LVH) by systolic blood pressure variability (BPV). *Logarithm of odds ratio.
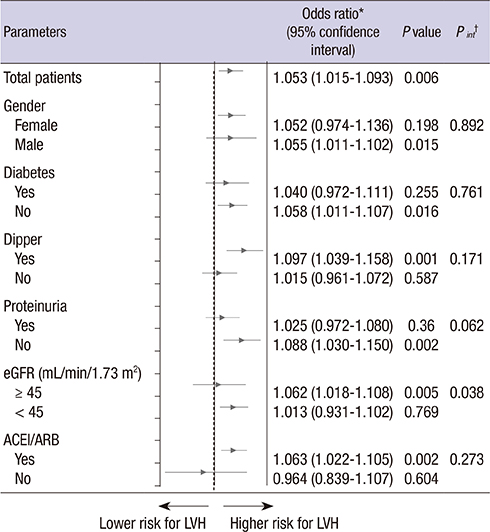
Fig. 2 The association* of blood pressure variability (BPV) and left ventricular hypertrophy (LVH) by subgroup. †ACEI/ARB, patients receiving an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker. *Logistic regression analysis: adjusted for age, sex, smoking, anti-hypertension medication use, 24-hr mean systolic blood pressure, diabetes, exercise, eGFR, and proteinuria (spot urine protein/creatinineratio [≥ 300 mg/g]). ‡Odds ratio; §95% confidence interval; ∥P value for the interaction between corresponding subgroups, as determined by logistic regression in the multivariable analysis.

Fig. 3 Odds ratio for left ventricular hypertrophy by systolic blood pressure variability (BPV) by the status of hypertension group. *Logarithm of odds ratio; †Hypertension groups by degree of controlled blood pressure (BP) (mmHg): True controlled group: Office BP (mmHg) < 140/80 and 24-hr BP < 135/85 (day) and 120/70 (night). White-coat effect group: Office BP (mmHg) ≥ 140/80 and 24-hr BP < 135/85 (day) and 120/70 (night). Masked hypertension group: Office BP (mmHg) < 140/80 and 24-hr BP ≥ 135/85 (day) or 120/70 (night). Sustained hypertension group: Office BP (mmHg) ≥ 140/80 and 24-hr BP ≥ 135/85 (day) and 120/70 (night). P value in each group: True controlled group, P = 0.055; White-coat effect group, P = 0.006; Masked hypertension group, P = 0.338; Sustained hypertension group, P = 0.077.
Reference
-
1. Rothwell PM. Limitations of the usual blood-pressure hypothesis and importance of variability, instability, and episodic hypertension. Lancet. 2010; 375:938–948.2. Okada H, Fukui M, Tanaka M, Inada S, Mineoka Y, Nakanishi N, Senmaru T, Sakabe K, Ushigome E, Asano M, et al. Visit-to-visit variability in systolic blood pressure is correlated with diabetic nephropathy and atherosclerosis in patients with type 2 diabetes. Atherosclerosis. 2012; 220:155–159.3. Poortvliet RK, Ford I, Lloyd SM, Sattar N, Mooijaart SP, de Craen AJ, Westendorp RG, Jukema JW, Packard CJ, Gussekloo J, et al. Blood pressure variability and cardiovascular risk in the PROspective Study of Pravastatin in the Elderly at Risk (PROSPER). PLoS One. 2012; 7:e52438.4. Mena L, Pintos S, Queipo NV, Aizpúrua JA, Maestre G, Sulbarán T. A reliable index for the prognostic significance of blood pressure variability. J Hypertens. 2005; 23:505–511.5. Muntner P, Shimbo D, Tonelli M, Reynolds K, Arnett DK, Oparil S. The relationship between visit-to-visit variability in systolic blood pressure and all-cause mortality in the general population: findings from NHANES III, 1988 to 1994. Hypertension. 2011; 57:160–166.6. Rothwell PM, Howard SC, Dolan E, O'Brien E, Dobson JE, Dahlöf B, Sever PS, Poulter NR. Prognostic significance of visit-to-visit variability, maximum systolic blood pressure, and episodic hypertension. Lancet. 2010; 375:895–905.7. McMullan CJ, Bakris GL, Phillips RA, Forman JP. Association of BP variability with mortality among African Americans with CKD. Clin J Am Soc Nephrol. 2013; 8:731–738.8. Di Iorio B, Pota A, Sirico ML, Torraca S, Di Micco L, Rubino R, Guastaferro P, Bellasi A. Blood pressure variability and outcomes in chronic kidney disease. Nephrol Dial Transplant. 2012; 27:4404–4410.9. Pringle E, Phillips C, Thijs L, Davidson C, Staessen JA, de Leeuw PW, Jaaskivi M, Nachev C, Parati G, O'Brien ET, et al. Systolic blood pressure variability as a risk factor for stroke and cardiovascular mortality in the elderly hypertensive population. J Hypertens. 2003; 21:2251–2257.10. Eguchi K, Hoshide S, Schwartz JE, Shimada K, Kario K. Visit-to-visit and ambulatory blood pressure variability as predictors of incident cardiovascular events in patients with hypertension. Am J Hypertens. 2012; 25:962–968.11. Schillaci G, Bilo G, Pucci G, Laurent S, Macquin-Mavier I, Boutouyrie P, Battista F, Settimi L, Desamericq G, Dolbeau G, et al. Relationship between short-term blood pressure variability and large-artery stiffness in human hypertension: findings from 2 large databases. Hypertension. 2012; 60:369–377.12. Diaz KM, Veerabhadrappa P, Kashem MA, Thakkar SR, Feairheller DL, Sturgeon KM, Ling C, Williamson ST, Kretzschmar J, Lee H, et al. Visit-to-visit and 24-h blood pressure variability: association with endothelial and smooth muscle function in African Americans. J Hum Hypertens. 2013; 27:671–677.13. Cha RH, Kim S, Ae Yoon S, Ryu DR, Eun Oh J, Han SY, Young Lee E, Ki Kim D, Kim YS. Association between blood pressure and target organ damage in patients with chronic kidney disease and hypertension: results of the APrODiTe study. Hypertens Res. 2014; 37:172–178.14. Lee CS, Cha RH, Lim YH, Kim H, Song KH, Gu N, Yu KS, Lim CS, Han JS, Kim S, et al. Ethnic coefficients for glomerular filtration rate estimation by the Modification of Diet in Renal Disease Study equations in the Korean population. J Korean Med Sci. 2010; 25:1616–1625.15. Romhilt DW, Estes EH Jr. A point-score system for the ECG diagnosis of left ventricular hypertrophy. Am Heart J. 1968; 75:752–758.16. Fagard R, Brguljan J, Thijs L, Staessen J. Prediction of the actual awake and asleep blood pressures by various methods of 24 h pressure analysis. J Hypertens. 1996; 14:557–563.17. Park SM, Ro YM, Ahn JC, Lim DS, Park CG, Kim YH, Seo HS, Shim WJ, Oh DJ. An appraisal of the electrocardiographic criteria for diagnosis of left ventricular hypertrophy in Koreans: comparison to echocardiographic measurement of left ventricular mass. Korean Circ J. 2004; 34:775–783.18. Price CP, Newall RG, Boyd JC. Use of protein:creatinine ratio measurements on random urine samples for prediction of significant proteinuria: a systematic review. Clin Chem. 2005; 51:1577–1586.19. Mancia G, Fagard R, Narkiewicz K, Redón J, Zanchetti A, Böhm M, Christiaens T, Cifkova R, De Backer G, Dominiczak A, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2013; 34:2159–2219.20. Ohkubo T, Kikuya M, Metoki H, Asayama K, Obara T, Hashimoto J, Totsune K, Hoshi H, Satoh H, Imai Y. Prognosis of "masked" hypertension and "white-coat" hypertension detected by 24-h ambulatory blood pressure monitoring 10-year follow-up from the Ohasama study. J Am Coll Cardiol. 2005; 46:508–515.21. Diaz KM, Veerabhadrappa P, Kashem MA, Feairheller DL, Sturgeon KM, Williamson ST, Crabbe DL, Brown MD. Relationship of visit-to-visit and ambulatory blood pressure variability to vascular function in African Americans. Hypertens Res. 2012; 35:55–61.22. Parati G, Pomidossi G, Albini F, Malaspina D, Mancia G. Relationship of 24-hour blood pressure mean and variability to severity of target-organ damage in hypertension. J Hypertens. 1987; 5:93–98.23. Hansen TW, Thijs L, Li Y, Boggia J, Kikuya M, Björklund-Bodegård K, Richart T, Ohkubo T, Jeppesen J, Torp-Pedersen C, et al. Prognostic value of reading-to-reading blood pressure variability over 24 hours in 8938 subjects from 11 populations. Hypertension. 2010; 55:1049–1057.24. Tatasciore A, Zimarino M, Renda G, Zurro M, Soccio M, Prontera C, Emdin M, Flacco M, Schillaci G, DE Caterina R. Awake blood pressure variability, inflammatory markers and target organ damage in newly diagnosed hypertension. Hypertens Res. 2008; 31:2137–2146.25. Abramson JL, Lewis C, Murrah NV, Anderson GT, Vaccarino V. Relation of C-reactive protein and tumor necrosis factor-alpha to ambulatory blood pressure variability in healthy adults. Am J Cardiol. 2006; 98:649–652.26. Kim KI, Lee JH, Chang HJ, Cho YS, Youn TJ, Chung WY, Chae IH, Choi DJ, Park KU, Kim CH. Association between blood pressure variability and inflammatory marker in hypertensive patients. Circ J. 2008; 72:293–298.27. Veerabhadrappa P, Diaz KM, Feairheller DL, Sturgeon KM, Williamson S, Crabbe DL, Kashem A, Ahrensfield D, Brown MD. Enhanced blood pressure variability in a high cardiovascular risk group of African Americans: FIT4Life Study. J Am Soc Hypertens. 2010; 4:187–195.28. Kawai T, Ohishi M, Ito N, Onishi M, Takeya Y, Yamamoto K, Kamide K, Rakugi H. Alteration of vascular function is an important factor in the correlation between visit-to-visit blood pressure variability and cardiovascular disease. J Hypertens. 2013; 31:1387–1395.29. Devereux RB, Casale PN, Eisenberg RR, Miller DH, Kligfield P. Electrocardiographic detection of left ventricular hypertrophy using echocardiographic determination of left ventricular mass as the reference standard: comparison of standard criteria, computer diagnosis and physician interpretation. J Am Coll Cardiol. 1984; 3:82–87.30. Hameed W, Razi MS, Khan MA, Hussain MM, Aziz S, Habib S, Aslam M. Electrocardiographic diagnosis of left ventricular hypertrophy: comparison with echocardiography. Pak J Physiol. 2005; 1:35–38.31. Jain A, Tandri H, Dalal D, Chahal H, Soliman EZ, Prineas RJ, Folsom AR, Lima JA, Bluemke DA. Diagnostic and prognostic utility of electrocardiography for left ventricular hypertrophy defined by magnetic resonance imaging in relationship to ethnicity: the Multi-Ethnic Study of Atherosclerosis (MESA). Am Heart J. 2010; 159:652–658.32. Miao CY, Xie HH, Zhan LS, Su DF. Blood pressure variability is more important than blood pressure level in determination of end-organ damage in rats. J Hypertens. 2006; 24:1125–1135.33. Theilade S, Lajer M, Jorsal A, Tarnow L, Parving HH, Rossing P. Arterial stiffness and endothelial dysfunction independently and synergistically predict cardiovascular and renal outcome in patients with type 1 diabetes. Diabet Med. 2012; 29:990–994.34. Kawai T, Ohishi M, Kamide K, Nakama C, Onishi M, Ito N, Takami Y, Takeya Y, Rakugi H. Differences between daytime and nighttime blood pressure variability regarding systemic atherosclerotic change and renal function. Hypertens Res. 2013; 36:232–239.35. KDIGO. KDIGO 2012 clinical practice guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl. 2013; 3:1–150.36. Fisher H, Hsu CY, Vittinghoff E, Lin F, Bansal N. Comparison of associations of urine protein-creatinine ratio versus albumin-creatinine ratio with complications of CKD: a cross-sectional analysis. Am J Kidney Dis. 2013; 62:1102–1108.37. Atkins RC, Briganti EM, Zimmet PZ, Chadban SJ. Association between albuminuria and proteinuria in the general population: the AusDiab Study. Nephrol Dial Transplant. 2003; 18:2170–2174.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hypertensive Retinopathy and Associated Target Organ Damage in Korean Hypertensive Patients
- Short-term blood pressure variability as a potential therapeutic target for kidney disease
- Carotid artery intima-media thickness and hypertensive heart disease: a short review
- 24 hour circadian pattern of blood pressure and its related target organ damage in hypertensive subjects
- Influence of Metabolic Syndrome on Hypertension-related Target Organ Damage: Diagnosis of Metabolic Syndrome Is Still Necessary
