State-of-the-Art CT Imaging Techniques for Congenital Heart Disease
- Affiliations
-
- 1Department of Radiology and the Research Institute of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul 138-736, Korea. hwgoo@amc.seoul.kr
- KMID: 1787009
- DOI: http://doi.org/10.3348/kjr.2010.11.1.4
Abstract
- CT is increasingly being used for evaluating the cardiovascular structures and airways in the patients with congenital heart disease. Multi-slice CT has traditionally been used for the evaluation of the extracardiac vascular and airway abnormalities because of its inherent high spatial resolution and excellent air-tissue contrast. Recent developments in CT technology primarily by reducing the cardiac motion and the radiation dose usage in congenital heart disease evaluation have helped expand the indications for CT usage. Tracheobronchomalacia associated with congenital heart disease can be evaluated with cine CT. Intravenous contrast injection should be tailored to unequivocally demonstrate cardiovascular abnormalities. Knowledge of the state-of-the-art CT imaging techniques that are used for evaluating congenital heart disease is helpful not only for planning and performing CT examinations, but also for interpreting and presenting the CT image findings that consequently guide the proper medical and surgical management.
MeSH Terms
Figure
-
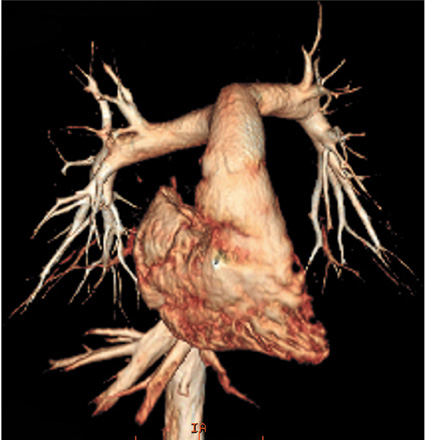
Fig. 1 Volume-rendered CT image with non-ECG-synchronized spiral scan shows excellent anatomic details of pulmonary arteries in 12-year-old girl with repaired coarctation of aorta.
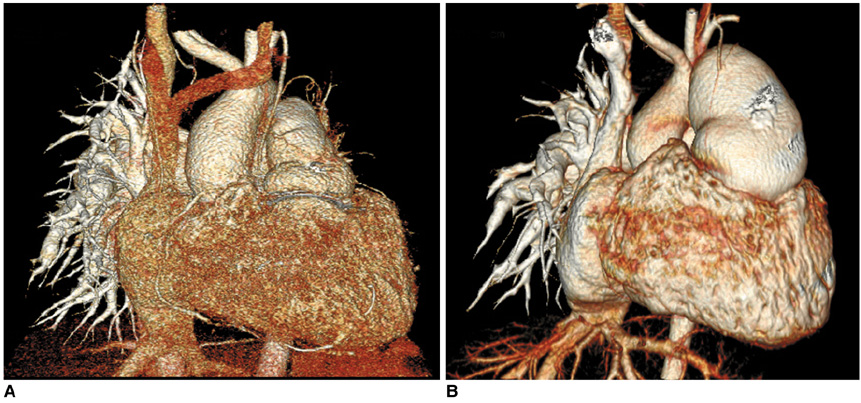
Fig. 2 Effect of slice thickness on image quality of non-ECG-synchronized spiral CT in 12-year-old boy with pulmonary atresia and ventricular septal defect after Rastelli operation. A. Volume-rendered CT image reconstructed from thin, overlapped axial images with 0.6-mm slice thickness at collimation of 0.6 mm appears quite grainy. That is because slice thickness is too thin at employed CT dose and this thin slice consequently increases image noise enough to degrade image quality. There are two ways to improve image quality in this situation: one is to slightly increase slice thickness and the other is to increase radiation dose a lot. B. Slight increase in slice thickness to 0.75 mm substantially improves image quality of volume-rendered CT image. This strategy is highly recommended because its dose saving effect is great.
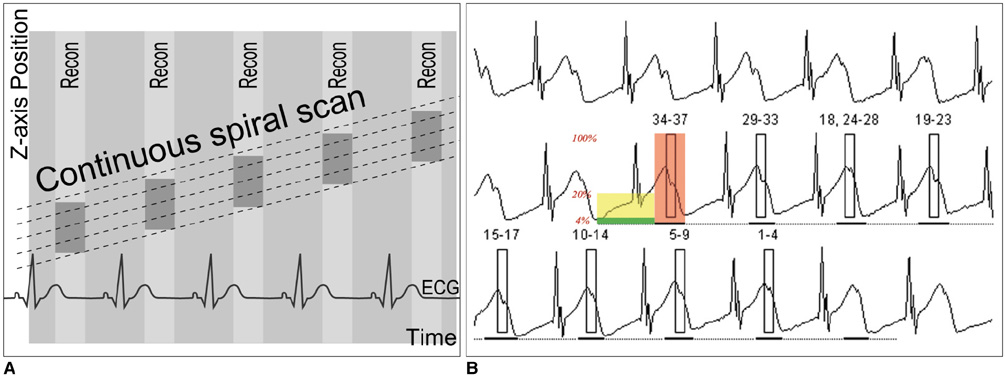
Fig. 3 Diagrams showing retrospective ECG-gated spiral CT scan. A. As demonstrated on schema, spiral scan is acquired with low enough pitch to avoid gap in CT data. This spiral CT data is retrospectively reconstructed at specific cardiac phase by synchronizing with simultaneously acquired ECG data. B. For ECG-controlled tube current modulation, period with 100% tube current should be appropriately determined depending on heart rates. End-systolic phase (red rectangle) is used at high heart rates. Tube current can be reduced to 20% (yellow rectangle) or 4% (light green rectangle) during rest of cardiac cycle.
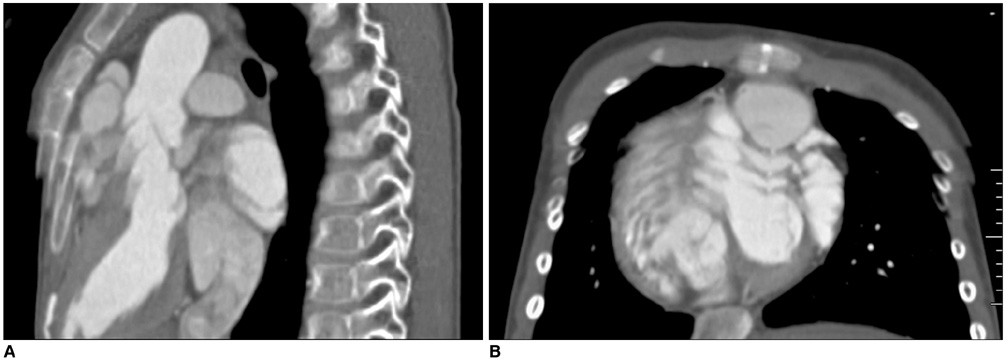
Fig. 4 6-year-old boy with repaired tetralogy of Fallot. Sagittal (A) and short-axis (B) retrospective ECG-gated spiral CT images, which are affected by severe respiratory motion artifacts, are shown at midportion of scan range.
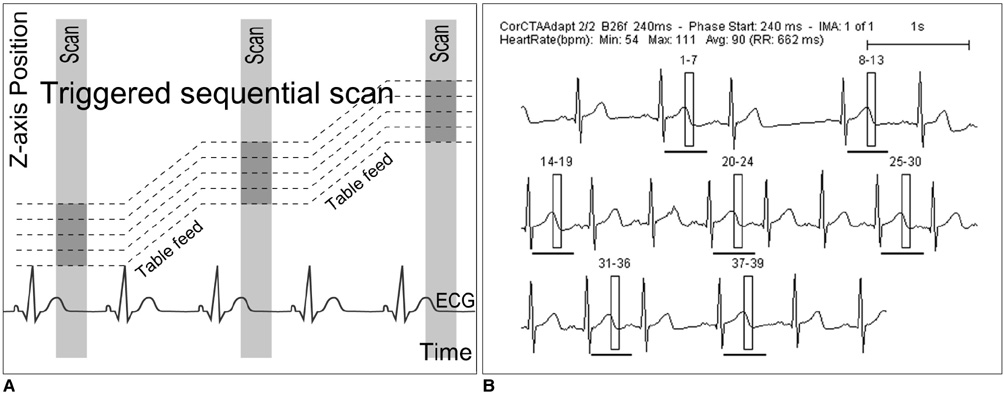
Fig. 5 Diagrams showing prospective ECG-triggered sequential CT scan. A. Sequential scan is acquired without table movement at predefined cardiac phase, which is end-systolic phase in this diagram. Then, time period is necessary to move CT table to next scan. Thus, scan mode is commonly called 'step and shoot' mode. B. ECG shows variable heart rates ranging from 54 bpm to 111 bpm. This variability in heart rates is commonly considered to be disadvantageous for performing prospective ECG-triggered sequential scan for mid-diastolic phase. However, this is not case when end-systolic phase is target. As demonstrated on this diagram, end-systolic phases can be consistently acquired at irregular heart rate with prospective ECG-triggered sequential scan. It should be noted that absolute delay, for instance, 240 ms in this case, must be used to have this benefit.
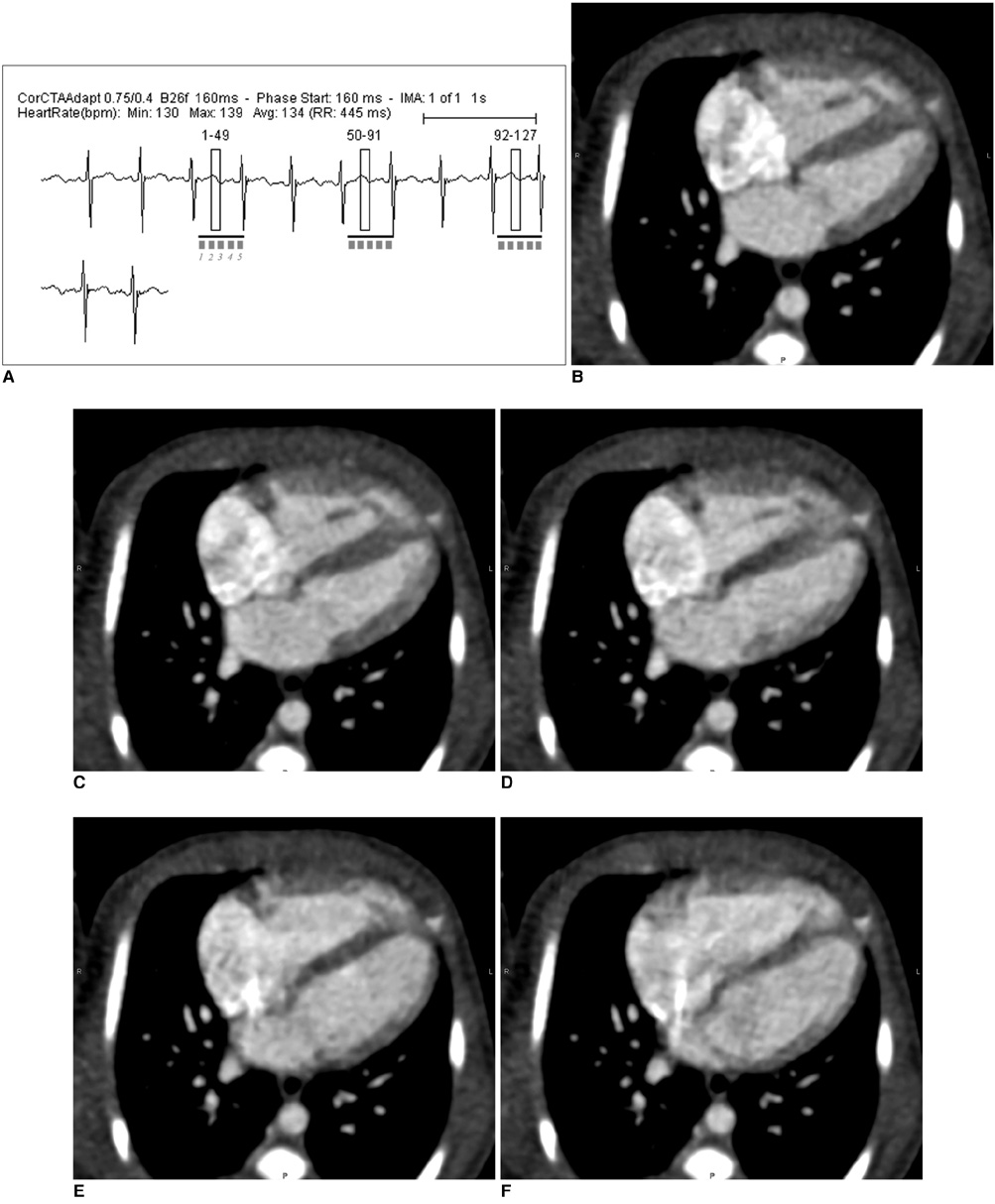
Fig. 6 Multi-phase prospective ECG-triggered sequential CT scan. A. Extended scan mode (0.38 s), in which period longer than necessary for single phase (0.2 s) is obtained, offers multi-phase study. Cardiac function can be evaluated with this scan mode at high heart rates (134 bpm in this case) because acquisition window covers both end-systole and end-diastole. B-F. After scan, five cardiac phases are retrospectively reconstructed at approximately 40-ms intervals (B, 160 ms; C, 200 ms; D, 240 ms; E, 280 ms; F 340 ms).
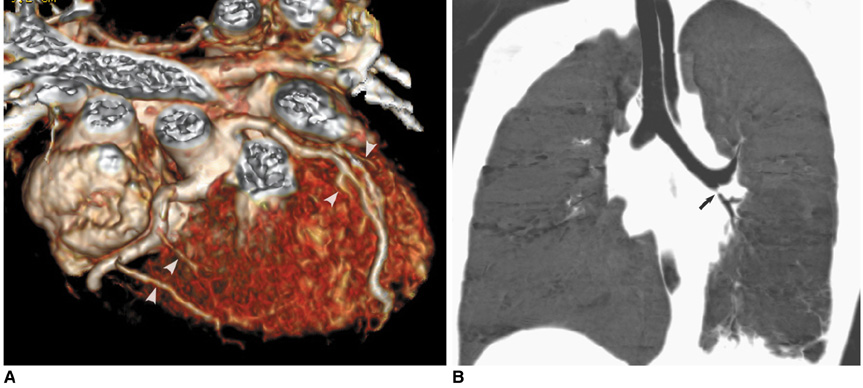
Fig. 7 Prospective ECG-triggered sequential CT scan in free-breathing young children is relatively less susceptible to respiratory motion artifacts than is retrospectively ECG-gated spiral CT scan. With this scan mode, even side-branches (arrowheads) of coronary arteries (A) and stenosis (arrow) involving left bronchi (B) are clearly delineated without cardiac and respiratory motion artifacts in young children. Therefore, more invasive or sophisticated preparation procedures such as general anesthesia or controlled ventilation are not currently needed for only diagnostic purposes.
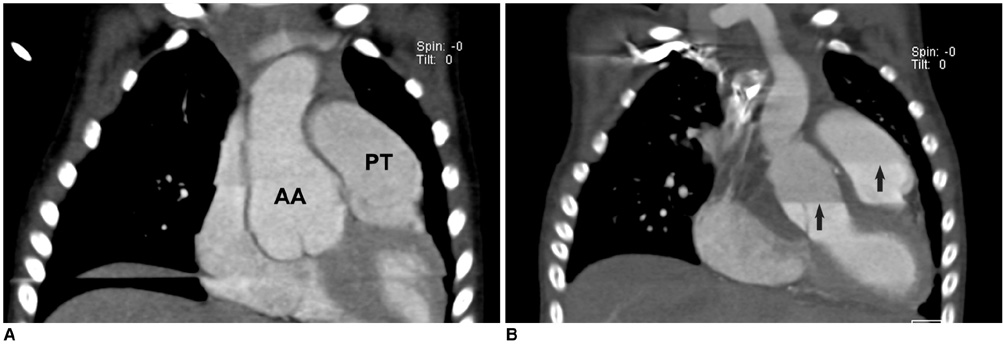
Fig. 8 Artifacts on prospective ECG-triggered sequential CT scan. A. Various degrees of stair-step artifacts derived from respiration motion are seen on coronal CT image. Artifacts are typically much more pronounced around diaphragm. Aneurysmal dilatations involving ascending aorta (AA) and pulmonary trunk (PT) are noted in 3-year-old girl with Loeys-Dietz syndrome. B. Stair-step artifacts on prospective ECG-triggered sequential coronal CT image are remarkably decreased by applying combined ECG and respiratory triggering for same patient who underwent valve sparing aortic root replacement surgery. In contrast, difference in cardiovascular enhancement is frequently observed between adjacent slabs (arrows) due to long examination time that is further lengthened by combined triggering.
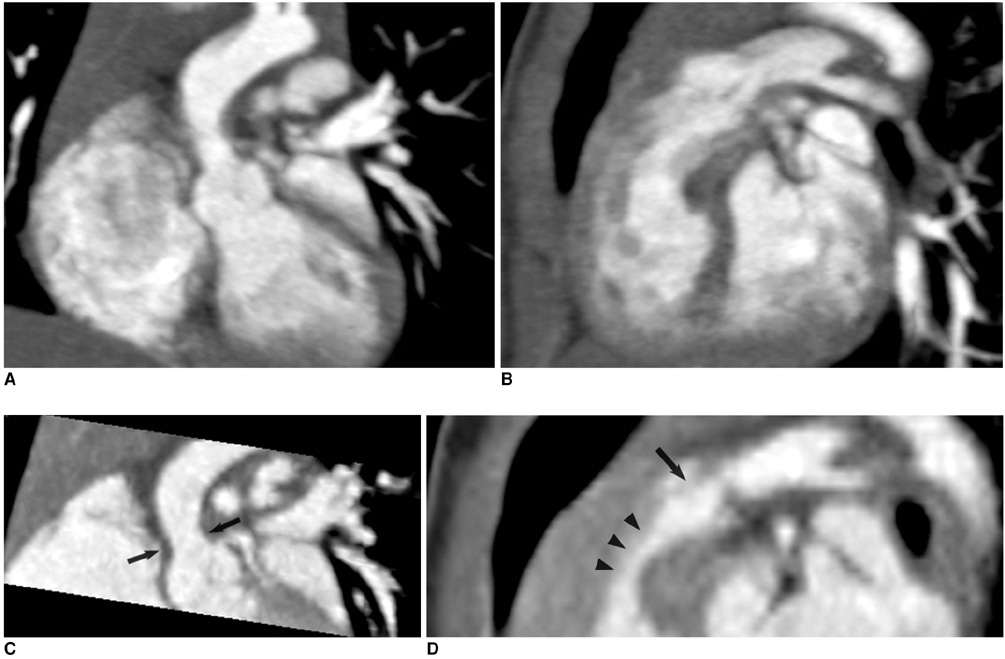
Fig. 9 Combo CT scan comprised of non-ECG-synchronized spiral scan with usual scan range (A, B) and prospective ECG-triggered sequential scan with narrow scan range confined to conotruncal area of heart (C, D) in 9-months-old boy with Williams syndrome. Supravalvular aortic stenosis (arrows on C) and combined valvar (arrow on D) and subvalvar (arrowheads on D) pulmonary stenoses are clearly shown on prospective ECG-triggered sequential CT images (C, D). Dose estimates are 1.6 mSv for non-ECG-synchronized spiral scan and 0.2 mSv for prospective ECG-triggered sequential scan.
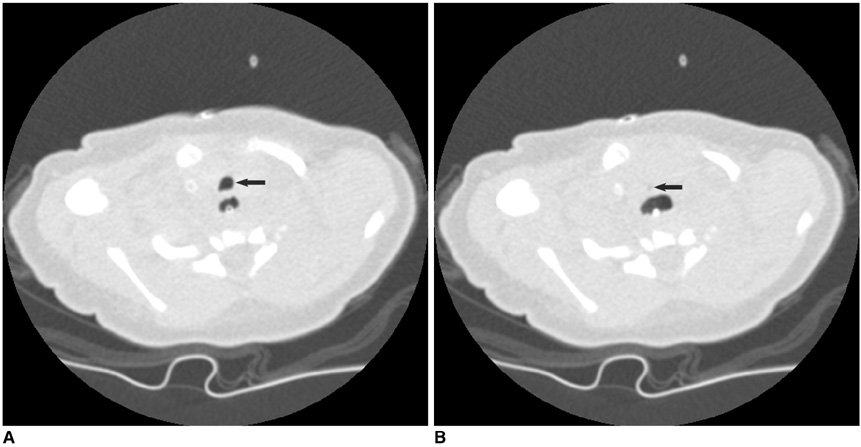
Fig. 10 Cine CT (A, inspiratory phase; B, expiratory phase) for diagnosis of tracheomalacia in 16-day-old female newborn with tracheoesophageal fistula, esophageal atresia and tetralogy of Fallot. Excessive expiratory collapsibility of trachea (arrows) is displayed on cine CT images. Distended proximal esophagus is also seen posterior to trachea.
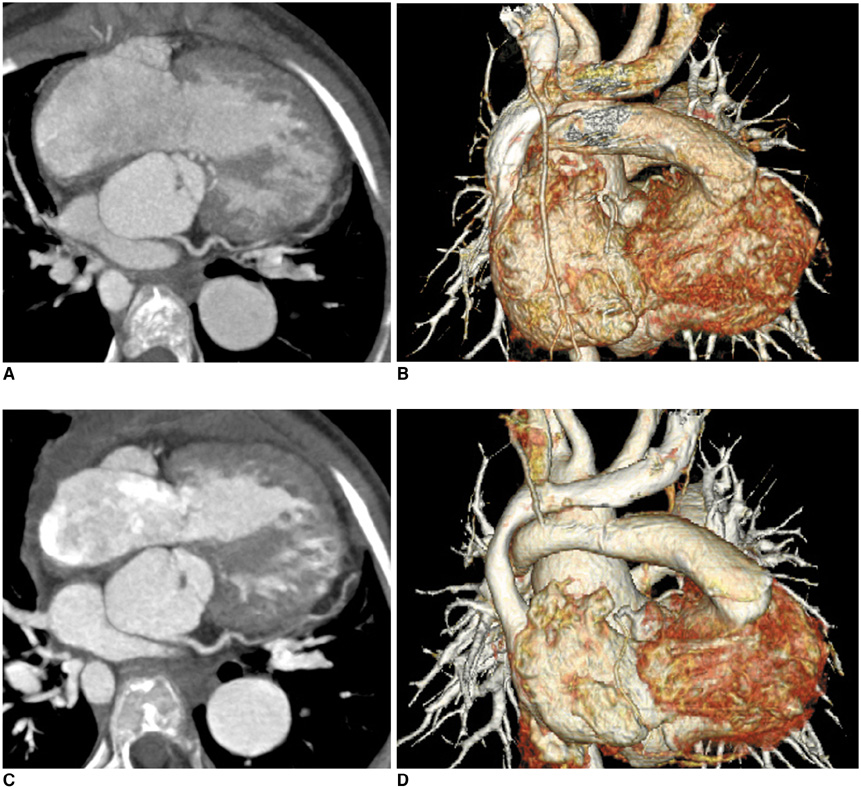
Fig. 11 Dose reduction by applying low kV and ECG-controlled tube current modulation to retrospective ECG-gated spiral CT scan in 9-year-old girl with pulmonary atresia, ventricular septal defect and major aortopulmonary collateral arteries and who underwent Rastelli operation. Dose estimate of CT scan acquired with 120 kV and conventional ECG pulsing (A, B) is 9.2 mSv (heart rate: 88 bpm). On other hand, dose estimate can be reduced to 3.5 mSv by applying 100 kV and MinDose for follow-up CT (heart rate: 86 bpm). Of interest, image quality of CT images is much better and degree of cardiovascular enhancement appears much higher on follow-up CT with lower radiation dose.
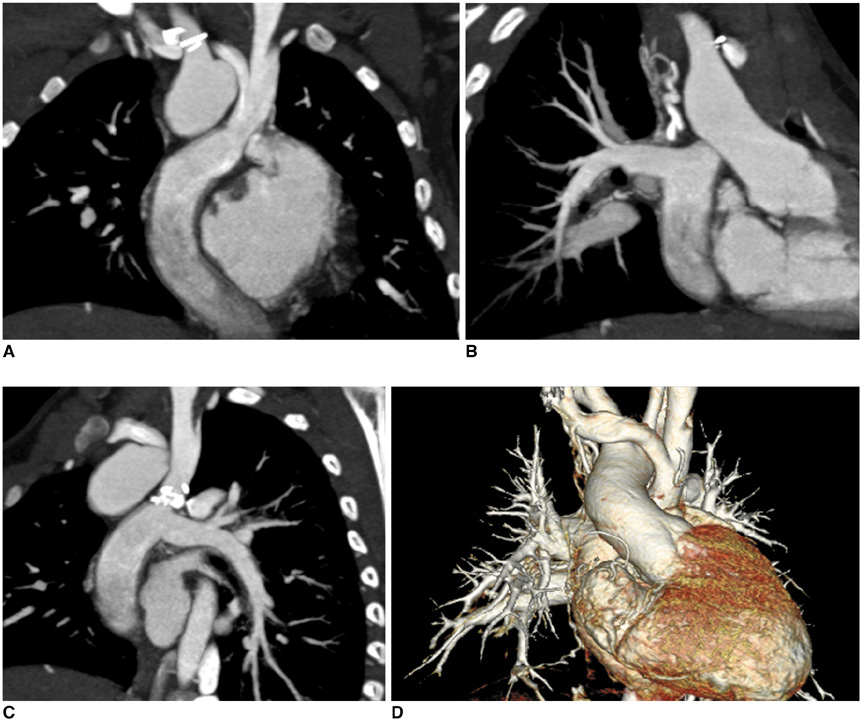
Fig. 12 Non-ECG-synchronized multiplanar reformatted (A-C) and volume-rendered (D) CT images clearly show patent Fontan pathway and pulmonary vessels in 5-year-old boy with functional single ventricle. Simultaneous intravenous injection of 50% diluted contrast agent through arm and leg veins was used to obtain homogeneously high enhancement of cardiovascular structures.
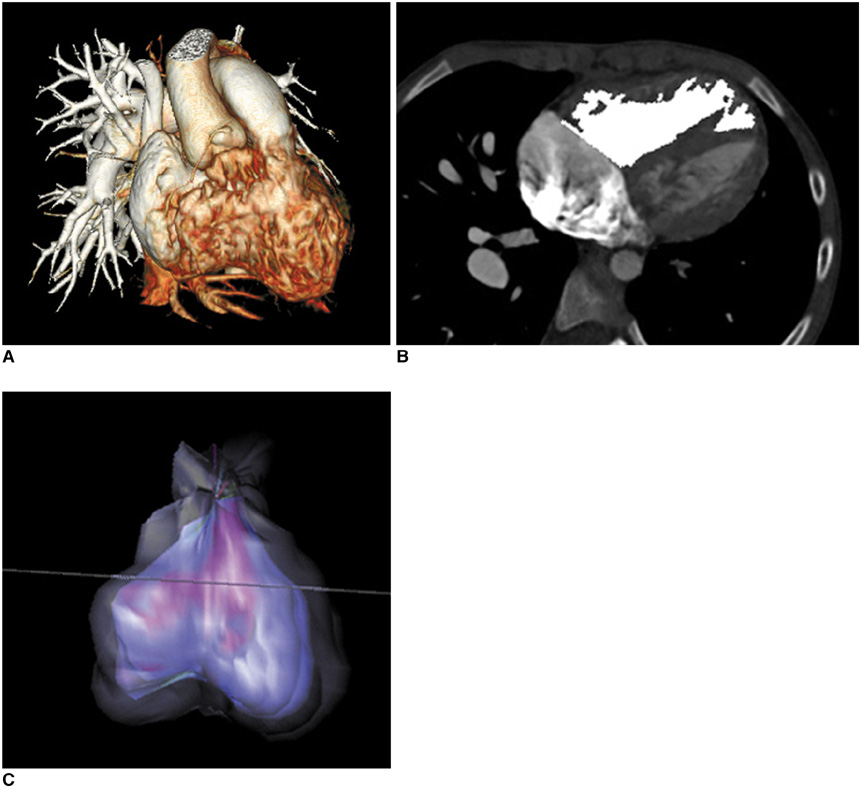
Fig. 13 Right ventricle CT volumetry in 8-year-old boy with repaired tetralogy of Fallot. Retrospective ECG-gated spiral CT was performed because of inconsistent right ventricle volumes on serial cardiac MR examinations (end-systolic volume of right ventricle was normalized to body surface area, 86 → 128 ml/m2). A. Crisp margin of right ventricle is shown with high spatial resolution on volume-rendered CT image. B, C. Consequently, right ventricular cavity can be accurately segmented with three-dimensional region growing method. End-systolic volume of right ventricle that's normalized to body surface area calculated with CT is 86 ml/m2, which indicates that volume at second cardiac MR examination is inaccurate.

Fig. 14 Dual-energy lung perfusion CT. In addition to pulmonary CT angiography (A), lung perfusion status (B) can be obtained without additional radiation dose by means of dual-energy CT technology when pulmonary thromboembolism is suspected in patients with congenital heart disease.
Cited by 10 articles
-
Advanced Medical Use of Three-Dimensional Imaging in Congenital Heart Disease: Augmented Reality, Mixed Reality, Virtual Reality, and Three-Dimensional Printing
Hyun Woo Goo, Sang Joon Park, Shi-Joon Yoo
Korean J Radiol. 2020;21(2):133-145. doi: 10.3348/kjr.2019.0625.Coronary Artery Imaging in Children
Hyun Woo Goo
Korean J Radiol. 2015;16(2):239-250. doi: 10.3348/kjr.2015.16.2.239.Combined Electrocardiography- and Respiratory-Triggered CT of the Lung to Reduce Respiratory Misregistration Artifacts between Imaging Slabs in Free-Breathing Children: Initial Experience
Hyun Woo Goo, Thomas Allmendinger
Korean J Radiol. 2017;18(5):860-866. doi: 10.3348/kjr.2017.18.5.860.Comparison of Chest Pain Protocols for Electrocardiography-Gated Dual-Source Cardiothoracic CT in Children and Adults: The Effect of Tube Current Saturation on Radiation Dose Reduction
Hyun Woo Goo
Korean J Radiol. 2018;19(1):23-31. doi: 10.3348/kjr.2018.19.1.23.Is It Better to Enter a Volume CT Dose Index Value before or after Scan Range Adjustment for Radiation Dose Optimization of Pediatric Cardiothoracic CT with Tube Current Modulation?
Hyun Woo Goo
Korean J Radiol. 2018;19(4):692-703. doi: 10.3348/kjr.2018.19.4.692.Computed Tomography Pulmonary Vascular Volume Ratio Can Be Used to Evaluate the Effectiveness of Pulmonary Angioplasty in Peripheral Pulmonary Artery Stenosis
Hyun Woo Goo
Korean J Radiol. 2019;20(10):1422-1430. doi: 10.3348/kjr.2019.0286.User-Friendly Vendor-Specific Guideline for Pediatric Cardiothoracic Computed Tomography Provided by the Asian Society of Cardiovascular Imaging Congenital Heart Disease Study Group: Part 1. Imaging Techniques
Sun Hwa Hong, Hyun Woo Goo, Eriko Maeda, Ki Seok Choo, I-Chen Tsai,
Korean J Radiol. 2019;20(2):190-204. doi: 10.3348/kjr.2018.0571.Diagnosis of Pulmonary Arterial Hypertension in Children by Using Cardiac Computed Tomography
Shyh-Jye Chen, Jou-Hsuan Huang, Wen-Jeng Lee, Ming-Tai Lin, Yih-Sharng Chen, Jou-Kou Wang
Korean J Radiol. 2019;20(6):976-984. doi: 10.3348/kjr.2018.0673.Quantification of Initial Right Ventricular Dimensions by Computed Tomography in Infants with Congenital Heart Disease and a Hypoplastic Right Ventricle
Hyun Woo Goo
Korean J Radiol. 2020;21(2):203-209. doi: 10.3348/kjr.2019.0662.CT-Based Essential Cardiac Residents to Understand Anatomy for Radiology Congenital Heart Disease
Hyun Woo Goo
J Korean Soc Radiol. 2019;80(6):1107-1120. doi: 10.3348/jksr.2019.80.6.1107.
Reference
-
1. Goo HW, Park IS, Ko JK, Kim YH, Seo DM, Yun TJ, et al. CT of congenital heart disease: normal anatomy and typical pathologic conditions. Radiographics. 2003. 23:S147–S165.2. Goo HW, Park IS, Ko JK, Kim YH, Seo DM, Park JJ. Computed tomography for the diagnosis of congenital heart disease in pediatric and adult patients. Int J Cardiovasc Imaging. 2005. 21:347–365.3. Leschka S, Oechslin E, Husmann L, Desbiolles L, Marincek B, Genoni M, et al. Pre- and postoperative evaluation of congenital heart disease in children and adults with 64-section CT. Radiographics. 2007. 27:829–846.4. Goo HW. Pediatric CT: understanding of radiation dose and optimization of imaging techniques. J Korean Radiol Soc. 2005. 52:1–5. [Korean].5. Yang DH, Goo HW. Pediatric 16-slice CT protocol: radiation dose and image quality. J Korean Radiol Soc. 2008. 59:333–347.6. Alkadhi H. Radiation dose of cardiac CT--what is the evidence? Eur Radiol. 2009. 19:1311–1315.7. Mayo JR, Leipsic JA. Radiation dose in cardiac CT. AJR Am J Roentgenol. 2009. 192:646–653.8. Ha HI, Goo HW, Seo JB, Song JW, Lee JS. Effects of high-resolution CT of the lung using partial versus full reconstruction on motion artifacts and image noise. AJR Am J Roentgenol. 2006. 187:618–622.9. Yang DH, Goo HW, Seo DM, Yun TJ, Park JJ, Park IS, et al. Multi-slice CT angiography of interrupted aortic arch. Pediatr Radiol. 2008. 38:89–100.10. Goo HW, Seo DM, Yun TJ, Park JJ, Park IS, Ko JK, et al. Coronary artery anomalies and clinically important anatomy in patients with congenital heart disease: multislice CT findings. Pediatr Radiol. 2009. 39:265–273.11. Tsai IC, Lee T, Chen MC, Fu YC, Jan SL, Wang CC, et al. Visualization of neonatal coronary arteries on multidetector row CT: ECG-gated versus non-ECG-gated technique. Pediatr Radiol. 2007. 37:818–825.12. Busch S, Johnson TR, Wintersperger BJ, Minaifar N, Bhargava A, Rist C, et al. Quantitative assessment of left ventricular function with dual-source CT in comparison to cardiac magnetic resonance imaging: initial findings. Eur Radiol. 2008. 18:570–575.13. Johnson TR, Nikolaou K, Wintersperger BJ, Leber AW, von Ziegler F, Rist C, et al. Dual-source CT cardiac imaging: initial experience. Eur Radiol. 2006. 16:1409–1415.14. Petersilka M, Bruder H, Krauss B, Stierstorfer K, Flohr TG. Technical principles of dual source CT. Eur J Radiol. 2008. 68:362–368.15. Kyriakou Y, Kachelriess M, Knaup M, Krause JU, Kalender WA. Impact of the z-flying focal spot on resolution and artifact behavior for a 64-slice spiral CT scanner. Eur Radiol. 2006. 16:1206–1215.16. Goo HW, Park IS, Ko JK, Kim YH, Seo DM, Yun TJ, et al. Visibility of the origin and proximal course of coronary arteries on non-ECG-gated heart CT in patients with congenital heart disease. Pediatr Radiol. 2005. 35:792–798.17. Tzedakis A, Damilakis J, Perisinakis K, Karantanas A, Karabekios S, Gourtsoyiannis N. Influence of z overscanning on normalized effective doses calculated for pediatric patients undergoing multidetector CT examinations. Med Phys. 2007. 34:1163–1175.18. Deak PD, Langner O, Lell M, Kalender WA. Effects of adaptive section collimation on patient radiation dose in multisection spiral CT. Radiology. 2009. 252:140–147.19. McCollough CH, Primak AN, Saba O, Bruder H, Stierstorfer K, Raupach R, et al. Dose performance of a 64-channel dual-source CT scanner. Radiology. 2007. 243:775–784.20. Ruzsics B, Gebregziabher M, Lee H, Brothers RL, Allmendinger T, Vogt S, et al. Coronary CT angiography: automatic cardiac-phase selection for image reconstruction. Eur Radiol. 2009. 19:1906–1913.21. Leschka S, Stolzmann P, Schmid FT, Scheffel H, Stinn B, Marincek B, et al. Low kilovoltage cardiac dual-source CT: attenuation, noise, and radiation dose. Eur Radiol. 2008. 18:1809–1817.22. Stolzmann P, Leschka S, Scheffel H, Krauss T, Desbiolles L, Plass A, et al. Dual-source CT in step-and-shoot mode: noninvasive coronary angiography with low radiation dose. Radiology. 2008. 249:71–80.23. Rybicki FJ, Otero HJ, Steigner ML, Vorobiof G, Nallamshetty L, Mitsouras D, et al. Initial evaluation of coronary images from 320-detector row computed tomography. Int J Cardiovasc Imaging. 2008. 24:535–546.24. Goo HW. Evaluation of the airways in patients with congenital heart disease using multislice CT. J Korean Pediatr Cardiol Soc. 2004. 8:37–43.25. Goo HW, Kim HJ. Detection of air trapping on inspiratory and expiratory phase images obtained by 0.3-second cine CT in the lungs of free-breathing young children. AJR Am J Roentgenol. 2006. 187:1019–1023.26. Jung YY, Goo HW. The optimal parameter for radiation dose in pediatric low dose abdominal CT: cross-sectional dimensions versus body weight. J Korean Radiol Soc. 2008. 58:169–175.27. van der Molen AJ, Geleijns J. Overranging in multisection CT: quantification and relative contribution to dose--comparison of four 16-section CT scanners. Radiology. 2007. 242:208–216.28. Lee CH, Goo JM, Ye HJ, Ye SJ, Park CM, Chun EJ, et al. Radiation dose modulation techniques in the multidetector CT era: from basics to practice. Radiographics. 2008. 28:1451–1459.29. Goo HW, Suh DS. Tube current reduction in pediatric non-ECG-gated heart CT by combined tube current modulation. Pediatr Radiol. 2006. 36:344–351.30. Goo HW, Suh DS. The influences of tube voltage and scan direction on combined tube current modulation: a phantom study. Pediatr Radiol. 2006. 36:833–840.31. Weustink AC, Mollet NR, Pugliese F, Meijboom WB, Nieman K, Heijenbrok-Kal MH, et al. Optimal electrocardiographic pulsing windows and heart rate: effect on image quality and radiation exposure at dual-source coronary CT angiography. Radiology. 2008. 248:792–798.32. Lee T, Tsai IC, Fu YC, Jan SL, Wang CC, Chang Y, et al. MDCT evaluation after closure of atrial septal defect with an Amplatzer septal occluder. AJR Am J Roentgenol. 2007. 188:W431–W439.33. Frush DP. Technique of pediatric thoracic CT angiography. Radiol Clin North Am. 2005. 43:419–433.34. Hollingsworth CL, Yoshizumi TT, Frush DP, Chan FP, Toncheva G, Nguyen G, et al. Pediatric cardiac-gated CT angiography: assessment of radiation dose. AJR Am J Roentgenol. 2007. 189:12–18.35. Bae KT. Peak contrast enhancement in CT and MR angiography: when does it occur and why? Pharmacokinetic study in a porcine model. Radiology. 2003. 227:809–816.36. Hopper KD, Mosher TJ, Kasales CJ, TenHave TR, Tully DA, Weaver JS. Thoracic spiral CT: delivery of contrast material pushed with injectable saline solution in a power injector. Radiology. 1997. 205:269–271.37. Litmanovitch D, Zamboni GA, Hauser TH, Lin PJ, Clouse ME, Raptopoulos V. ECG-gated chest CT angiography with 64-MDCT and tri-phasic IV contrast administration regimen in patients with acute non-specific chest pain. Eur Radiol. 2008. 18:308–317.38. Eichhorn JG, Jourdan C, Hill SL, Raman SV, Cheatham JP, Long FR. CT of pediatric vascular stents used to treat congenital heart disease. AJR Am J Roentgenol. 2008. 190:1241–1246.39. Jhang WK, Park JJ, Seo DM, Goo HW, Gwak M. Perioperative evaluation of airways in patients with arch obstruction and intracardiac defects. Ann Thorac Surg. 2008. 85:1753–1758.40. Goo HW, Jhang WK, Kim YH, Ko JK, Park IS, Park JJ, et al. CT findings of plastic bronchitis in children after Fontan operation. Pediatr Radiol. 2008. 38:989–993.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- CT-Based Essential Cardiac Anatomy for Radiology Residents to Understand Congenital Heart Disease
- Imaging of Congenital Heart Disease in Hong Kong: From Invasive to Non-invasive Cardiac Imaging
- Dynamic CT Perfusion Imaging: State of the Art
- User-Friendly Vendor-Specific Guideline for Pediatric Cardiothoracic Computed Tomography Provided by the Asian Society of Cardiovascular Imaging Congenital Heart Disease Study Group: Part 1. Imaging Techniques
- Special Report: A 21-Year Publication Analysis of Congenital Heart CT and MRI Articles
