Planimetric Measurement of the Regurgitant Orifice Area Using Multidetector CT for Aortic Regurgitation: a Comparison with the Use of Echocardiography
- Affiliations
-
- 1Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 135-710, Korea. yhchoe@skku.edu
- 2Department of Radiology, Chungbuk National University Hospital, College of Medicine and Medical Research Institute, Chungbuk National University, Cheongju, Chungbuk 561-712, Korea.
- 3Cardiovascular Imaging Center, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 135-710, Korea.
- 4Division of Cardiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 135-710, Korea.
- 5Department of Thoracic and Cardiovascular Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 135-710, Korea.
- 6Division of Cardiology, Department of Internal Medicine, Mayo Clinic, Mayo Clinic College of Medicine, Rochester, MN, USA.
- KMID: 1783193
- DOI: http://doi.org/10.3348/kjr.2010.11.2.169
Abstract
OBJECTIVE
This study compared the area of the regurgitant orifice, as measured by the use of multidetector-row CT (MDCT), with the severity of aortic regurgitation (AR) as determined by the use of echocardiography for AR.
MATERIALS AND METHODS
In this study, 45 AR patients underwent electrocardiography-gated 40-slice or 64-slice MDCT and transthoracic or transesophageal echocardiography. We reconstructed CT data sets during mid-systolic to enddiastolic phases in 10% steps (20% and 35-95% of the R-R interval), planimetrically measuring the abnormally opened aortic valve area during diastole on CT reformatted images and comparing the area of the aortic regurgitant orifice (ARO) so measured with the severity of AR, as determined by echocardiography.
RESULTS
In the 14 patients found to have mild AR, the ARO area was 0.18+/-0.13 cm2 (range, 0.04-0.54 cm2). In the 15 moderate AR patients, the ARO area was 0.36 +/- 0.23 cm2 (range, 0.09-0.81 cm2). In the 16 severe AR patients, the ARO area was 1.00 +/- 0.51 cm2 (range, 0.23-1.84 cm2). Receiver-operator characteristic curve analysis determined a sensitivity of 85% and a specificity of 82%, for a cutoff of 0.47 cm2, to distinguish severe AR from less than severe AR with the use of CT (area under the curve = 0.91; 95% confidence interval, 0.84-1.00; p < 0.001).
CONCLUSION
Planimetric measurement of the ARO area using MDCT is useful for the quantitative evaluation of the severity of aortic regurgitation.
MeSH Terms
-
Adolescent
Adult
Aged
Aged, 80 and over
Aortic Valve/physiopathology/radiography/ultrasonography
Aortic Valve Insufficiency/*radiography/*ultrasonography
Area Under Curve
Body Weights and Measures/methods
Echocardiography/methods
Echocardiography, Doppler, Color/methods
Echocardiography, Transesophageal/methods
Electrocardiography
Female
Humans
Male
Middle Aged
ROC Curve
Retrospective Studies
Sensitivity and Specificity
Severity of Illness Index
Tomography, X-Ray Computed/*methods
Young Adult
Figure
-

Fig. 1 Demonstration of CT raw data reconstruction and aortic regurgitant orifice measurement at workstation, in 71-year-old male patient with moderate aortic regurgitation shown by transthoracic echocardiography. In this particular patient, image reconstruction was performed in 5% steps instead of 10% steps of our CT protocol. A. Aortic valve area was chosen from CT scout image to reconstruct images of multiple cardiac phases. B. Short-axial images of aortic valve, showing exact regurgitant orifice area produced from two orthogonal aortic longitudinal planes. C. Resultant aortic valve short-axial images in multiple planes (5-95% in 5% steps) show almost same regurgitant areas of aortic valve during diastolic phases. Image quality is excellent during mid-diastole (65-85%). D, E. In this case, aortic regurgitant orifice area via CT measured 0.31 cm2. Vena contracta, effective regurgitant orifice, and pressure half-time at echocardiography were 0.44 cm, 0.30 cm2, and 272 ms, respectively.
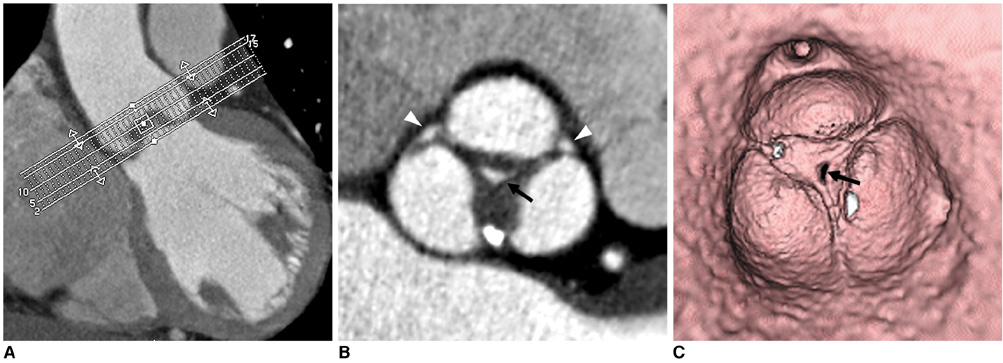
Fig. 2 60-year-old male with mild central aortic regurgitation shown by transthoracic echocardiography. A. Image shows batch reconstruction of aortic valve short-axial images in 1 mm thicknesses and 1 mm intervals. B. Resultant image visualizes central coaptation failure zone of 0.17 cm2 (arrow) and fusion of left and noncoronary cusps. Small areas of coaptation failure in peripheral commissure of aortic valve were suspected (arrowheads). C. Virtual angioscopic image confirms central regurgitation area (arrow). However, there was no evidence of commissural incompetency in periphery.
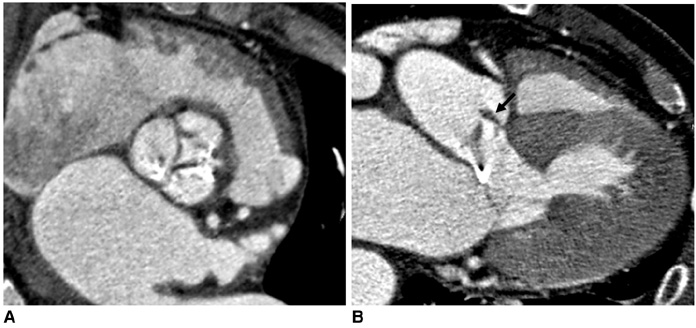
Fig. 3 76-year-old male with infective endocarditis and moderate eccentric aortic regurgitation and stenosis shown by transthoracic echocardiography. A. Reformatted image shows diastolic coaptation failure with valvular thickening and calcifications. Aortic regurgitant orifice at CT was 0.64 cm2. B. Long-axial image of aortic valve demonstrates 0.5 cm-vegetation (arrow) attached to valve leaflet. Vena contracta was 0.43 cm, and pressure half-time measured 183 ms at echocardiography.
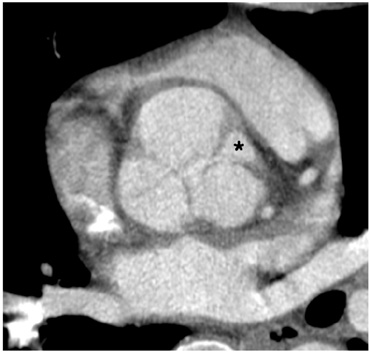
Fig. 4 37-year-old male with severe aortic regurgitation shown by transthoracic echocardiography. Reformatted CT image shows large area (asterisk) of commissural incompetency between right and left coronary cusps. Aortic regurgitant orifice area via CT measured 1.49 cm2. Effective regurgitant orifice area was 0.82 cm2 and pressure half-time, 259 ms at echocardiography.
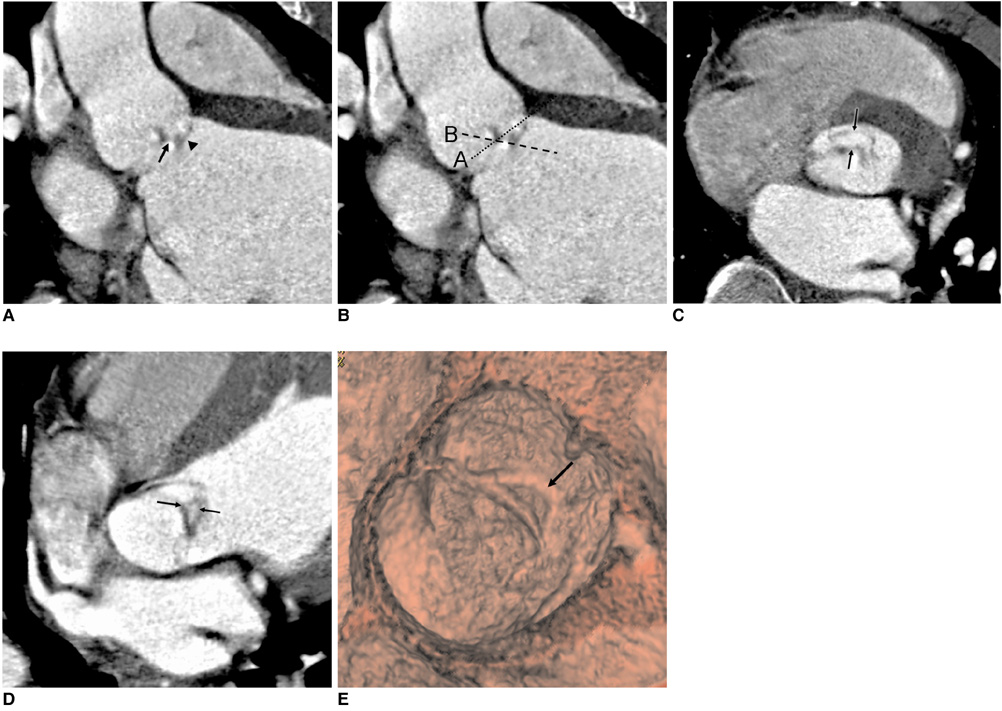
Fig. 5 38-year-old male with right coronary cusp prolapse and eccentric aortic regurgitation. A. Reformatted image shows prolapsed right coronary cusp (arrowhead) and coaptation failure of aortic valve (arrow). B. Dotted lines A and B indicate image reconstruction planes for central aortic regurgitation and eccentric aortic regurgitation with prolapsed cusp, respectively. C. Image reconstructed along plane A shows ovoid area (between arrows), indicating prolapsed part of right coronary cusp, not aortic regurgitant orifice. D. Image reconstructed along plane B shows aortic regurgitant orifice (between arrows). E. Virtual angioscopic image shows eccentric aortic regurgitant orifice (arrow).
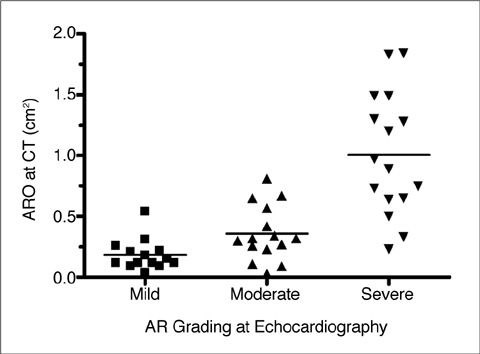
Fig. 6 Scatter plot of data shows significant difference in aortic regurgitant orifice area via CT between patients with severe AR and those with mild to moderate AR, determined with use of transthoracic echocardiography. AR = aortic regurgitation, ARO = aortic regurgitant orifice

Fig. 7 Receiver operation characteristic curve analysis shows accuracy of aortic regurgitant orifice area via CT in discriminating mild aortic regurgitation from moderate to severe aortic regurgitation (A) and mild to moderate aortic regurgitation from severe aortic regurgitation (B). Optimal cutoff values for mid aortic regurgitation and severe aortic regurgitation were 0.27 cm2 and 0.47 cm2, respectively. ARO = aortic regurgitant orifice
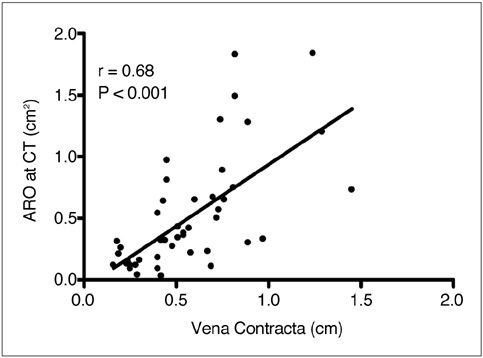
Fig. 8 Correlation between aortic regurgitant orifice area via CT and vena contracta width shown by transthoracic echocardiography (r = 0.68, p < 0.001). ARO = aortic regurgitant orifice
Cited by 1 articles
-
Morphological and Functional Evaluation of Quadricuspid Aortic Valves Using Cardiac Computed Tomography
Inyoung Song, Jung Ah Park, Bo Hwa Choi, Sung Min Ko, Je Kyoun Shin, Hyun Keun Chee, Jun Seok Kim
Korean J Radiol. 2016;17(4):463-471. doi: 10.3348/kjr.2016.17.4.463.
Reference
-
1. Enriquez-Sarano M, Tajik AJ. Clinical practice. Aortic regurgitation. N Engl J Med. 2004. 351:1539–1546.2. Bekeredjian R, Grayburn PA. Valvular heart disease: aortic regurgitation. Circulation. 2005. 112:125–134.3. Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD, Levine RA, et al. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr. 2003. 16:777–802.4. Tribouilloy CM, Enriquez-Sarano M, Bailey KR, Seward JB, Tajik AJ. Assessment of severity of aortic regurgitation using the width of the vena contracta: a clinical color Doppler imaging study. Circulation. 2000. 102:558–564.5. Eren M, Eksik A, Gorgulu S, Norgaz T, Dagdeviren B, Bolca O, et al. Determination of vena contracta and its value in evaluating severity of aortic regurgitation. J Heart Valve Dis. 2002. 11:567–575.6. Mascherbauer J, Rosenhek R, Bittner B, Binder J, Simon P, Maurer G, et al. Doppler echocardiographic assessment of valvular regurgitation severity by measurement of the vena contracta: an in vitro validation study. J Am Soc Echocardiogr. 2005. 18:999–1006.7. Fang L, Hsiung MC, Miller AP, Nanda NC, Yin WH, Young MS, et al. Assessment of aortic regurgitation by live three-dimensional transthoracic echocardiographic measurements of vena contracta area: usefulness and validation. Echocardiography. 2005. 22:775–781.8. Mizushige K, Nozaki S, Ohmori K, Matsuo H. Evaluation of effective aortic regurgitant orifice area and its effect on aortic regurgitant volume with Doppler echocardiography. Angiology. 2000. 51:241–246.9. Alkadhi H, Wildermuth S, Bettex DA, Plass A, Baumert B, Leschka S, et al. Mitral regurgitation: quantification with 16-detector row CT-initial experience. Radiology. 2006. 238:454–463.10. Gilkeson RC, Markowitz AH, Balgude A, Sachs PB. MDCT evaluation of aortic valvular disease. AJR Am J Roentgenol. 2006. 186:350–360.11. Alkadhi H, Wildermuth S, Plass A, Bettex D, Baumert B, Leschka S, et al. Aortic stenosis: comparative evaluation of 16-detector row CT and echocardiography. Radiology. 2006. 240:47–55.12. Habis M, Daoud B, Roger VL, Ghostine S, Caussin C, Ramadan R, et al. Comparison of 64-slice computed tomography planimetry and Doppler echocardiography in the assessment of aortic valve stenosis. J Heart Valve Dis. 2007. 16:216–224.13. Feuchtner GM, Müller S, Bonatti J, Schachner T, Velik-Salchner C, Pachinger O, et al. Sixty-four slice CT evaluation of aortic stenosis using planimetry of the aortic valve area. AJR Am J Roentgenol. 2007. 189:197–203.14. Pouleur AC, le Polain de Waroux JB, Pasquet A, Vanoverschelde JL, Gerber BL. Aortic valve area assessment: multidetector CT compared with cine MR imaging and transthoracic and transesophageal echocardiography. Radiology. 2007. 244:745–754.15. Vogel-Claussen J, Pannu H, Spevak PJ, Fishman EK, Bluemke DA. Cardiac valve assessment with MR imaging and 64-section multi-detector row CT. Radiographics. 2006. 26:1769–1784.16. Ryan R, Abbara S, Colen RR, Arnous S, Quinn M, Cury RC, et al. Cardiac valve disease: spectrum of findings on cardiac 64-MDCT. AJR Am J Roentgenol. 2008. 190:W294–W303.17. Alkadhi H, Desbiolles L, Husmann L, Plass A, Leschka S, Scheffel H, et al. Aortic regurgitation: assessment with 64-section CT. Radiology. 2007. 245:111–121.18. Jassal DS, Shapiro MD, Neilan TG, Chaithiraphan V, Ferencik M, Teague SD, et al. 64-slice multidetector computed tomography (MDCT) for detection of aortic regurgitation and quantification of severity. Invest Radiol. 2007. 42:507–512.19. Goffinet C, Kersten V, Pouleur AC, le Polain de Waroux JB, Vancraeynest D, Pasquet A, et al. Comprehensive assessment of the severity and mechanism of aortic regurgitation using multidetector CT and MR. Eur Radiol. 2010. 20:326–336.20. Li X, Tang L, Zhou L, Duan Y, Yanhui S, Yang R, et al. Aortic valves stenosis and regurgitation: assessment with dual source computed tomography. Int J Cardiovasc Imaging. 2009. 25:591–600.21. Feuchtner GM, Dichtl W, Müller S, Jodocy D, Schachner T, Klauser A, et al. 64-MDCT for diagnosis of aortic regurgitation in patients referred to CT coronary angiography. AJR Am J Roentgenol. 2008. 191:W1–W7.22. Feuchtner GM, Dichtl W, Schachner T, Müller S, Mallouhi A, Friedrich GJ, et al. Diagnostic performance of MDCT for detecting aortic valve regurgitation. AJR Am J Roentgenol. 2006. 186:1676–1681.23. Tribouilloy CM, Enriquez-Sarano M, Fett SL, Bailey KR, Seward JB, Tajik AJ. Application of the proximal flow convergence method to calculate the effective regurgitant orifice area in aortic regurgitation. J Am Coll Cardiol. 1998. 32:1032–1039.24. Zoghbi WA, Farmer KL, Soto JG, Nelson JG, Quinones MA. Accurate noninvasive quantification of stenotic aortic valve area by Doppler echocardiography. Circulation. 1986. 73:452–459.25. Bartunek J, De Bacquer D, Rodrigues AC, De Bruyne B. Accuracy of aortic stenosis severity assessment by Doppler echocardiography: importance of image quality. Int J Card Imaging. 1995. 11:97–104.26. Danielsen R, Nordrehaug JE, Vik-Mo H. Factors affecting Doppler echocardiographic valve area assessment in aortic stenosis. Am J Cardiol. 1989. 63:1107–1111.27. Ozkan M, Ozdemir N, Kaymaz C, Kirma C, Deligönül U. Measurement of aortic valve anatomic regurgitant area using transesophageal echocardiography: implications for the quantitation of aortic regurgitation. J Am Soc Echocardiogr. 2002. 15:1170–1174.28. Masci PG, Dymarkowski S, Bogaert J. Valvular heart disease: what does cardiovascular MRI add? Eur Radiol. 2008. 18:197–208.29. Gelfand EV, Hughes S, Hauser TH, Yeon SB, Goepfert L, Kissinger KV, et al. Severity of mitral and aortic regurgitation as assessed by cardiovascular magnetic resonance: optimizing correlation with Doppler echocardiography. J Cardiovasc Magn Reson. 2006. 8:503–507.30. Kutty S, Whitehead KK, Natarajan S, Harris MA, Wernovsky G, Fogel MA. Qualitative echocardiographic assessment of aortic valve regurgitation with quantitative cardiac magnetic resonance: a comparative study. Pediatr Cardiol. 2009. 30:971–977.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Quantitative Evaluation of Regurgitant Volume in the Patients with Mitral Regurgitation Using Color Doppler Proximal Isovelocity Surface Area Method
- Assessment of Aortic Regurgitation by Real-time Two-dimensional Doppler Flow Mapping System
- Comparison of Cine Magnetic Resonance Imaging with Doppler Echocardiography for the Quantative Evaluation of Tricuspid Regurgitation in Newborn
- Color Doppler Assessment of Mitral Regurgitation
- Morphological and Functional Evaluation of Quadricuspid Aortic Valves Using Cardiac Computed Tomography
