MR Imaging of Orbital Inflammatory Pseudotumors with Extraorbital Extension
- Affiliations
-
- 1Department of Radiology, College of Medicine, Myongji Hospital, Kwandong University of Korea. ejl1048@hanmail.net
- 2Department of Radiology, College of Medicine, The Catholic University of Korea, Korea.
- 3Department of Radiology, Gacheon Medical College, Gil Medical Center, Korea.
- KMID: 1783180
- DOI: http://doi.org/10.3348/kjr.2005.6.2.82
Abstract
OBJECTIVE
To demonstrate a variety of MR imaging findings of orbital inflammatory pseudotumors with extraorbital extension. MATERIALS AND METHODS: We retrospectively reviewed the MR features of five patients, who were diagnosed clinically and radiologically as having an orbital inflammatory pseudotumor with extraorbital extension. RESULTS: The types of orbital pseudotumors were a mass in the orbital apex (n = 3), diffuse form (n = 2), and myositis (n = 1). The extraorbital extension of the orbital pseudotumor passed through the superior orbital fissure in all cases, through the inferior orbital fissure in two cases, and through the optic canal in one case. The orbital lesions extended into the following areas: the cavernous sinus (n = 4), the middle cranial fossa (n = 4), Meckel's cave (n = 2), the petrous apex (n = 2), the clivus (n = 2), the pterygopalatine fossa and infratemporal fossa (n = 2), the foramen rotundum (n = 1), the paranasal sinus (n = 1), and the infraorbital foramen (n = 1). On MR imaging, the lesions appeared as an isosignal intensity with gray matter on the T1-weighted images, as a low signal intensity on the T2-weighted images and showed a marked enhancement on the post-gadolinium-diethylene triamine pentaacetic acid (post-Gd-DTPA) T1-sequences. The symptoms of all of the patients improved when they were given high doses of steroids. Three of the five patients experienced a recurrence. CONCLUSION: MR imaging is useful for demonstrating the presence of a variety of extraorbital extensions of orbital inflammatory pseudotumors.
Keyword
MeSH Terms
Figure
-
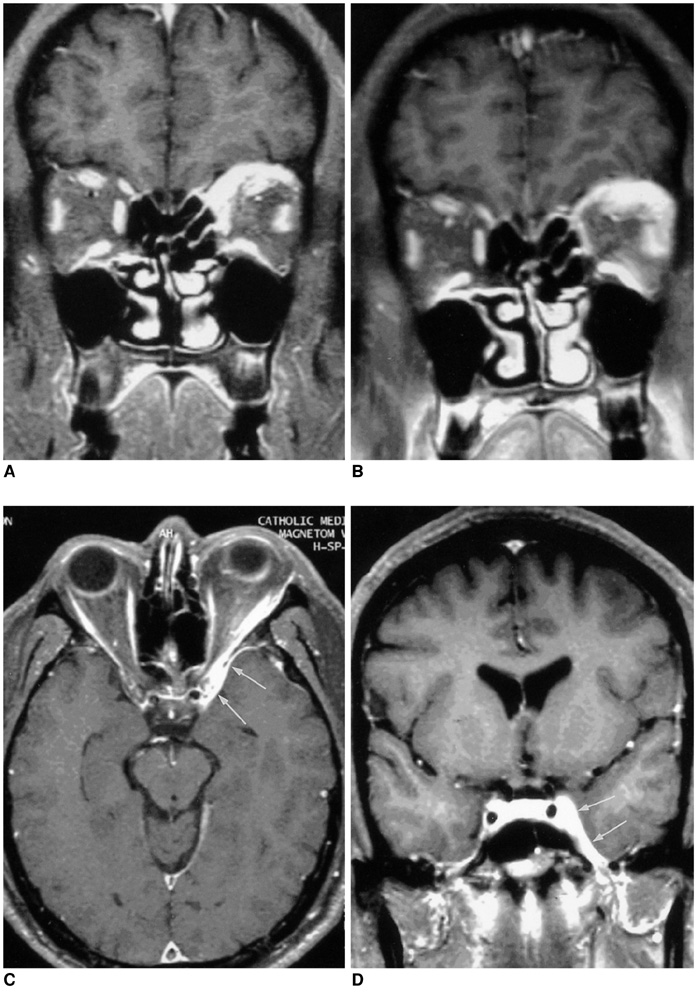
Fig. 1 Case 1. A 58-year-old man with diplopia and trigeminal neuralgia. A. An initial MR image with fat suppressed postcontrast coronal T1-weighted images shows increased thickness of the left rectus muscles with dense contrast enhancement, combined with a soft tissue mass in the superomedial aspect of the extra-conal space. A mild infiltration into the left orbital fat is also noted. The symptoms improved after steroid treatment. B-D. Follow-up MR images obtained after five months. Postcontrast T1-weighted images with fat suppression show a recurrence. Diffuse infiltrating enhancement in the left orbital fossa and apex is seen along ith an increase in the thickness of the rectus muscles; this extends posteriorly through the superior orbital fissure into the left cavernous sinus and adjacent temporal pachymeninges (arrows).
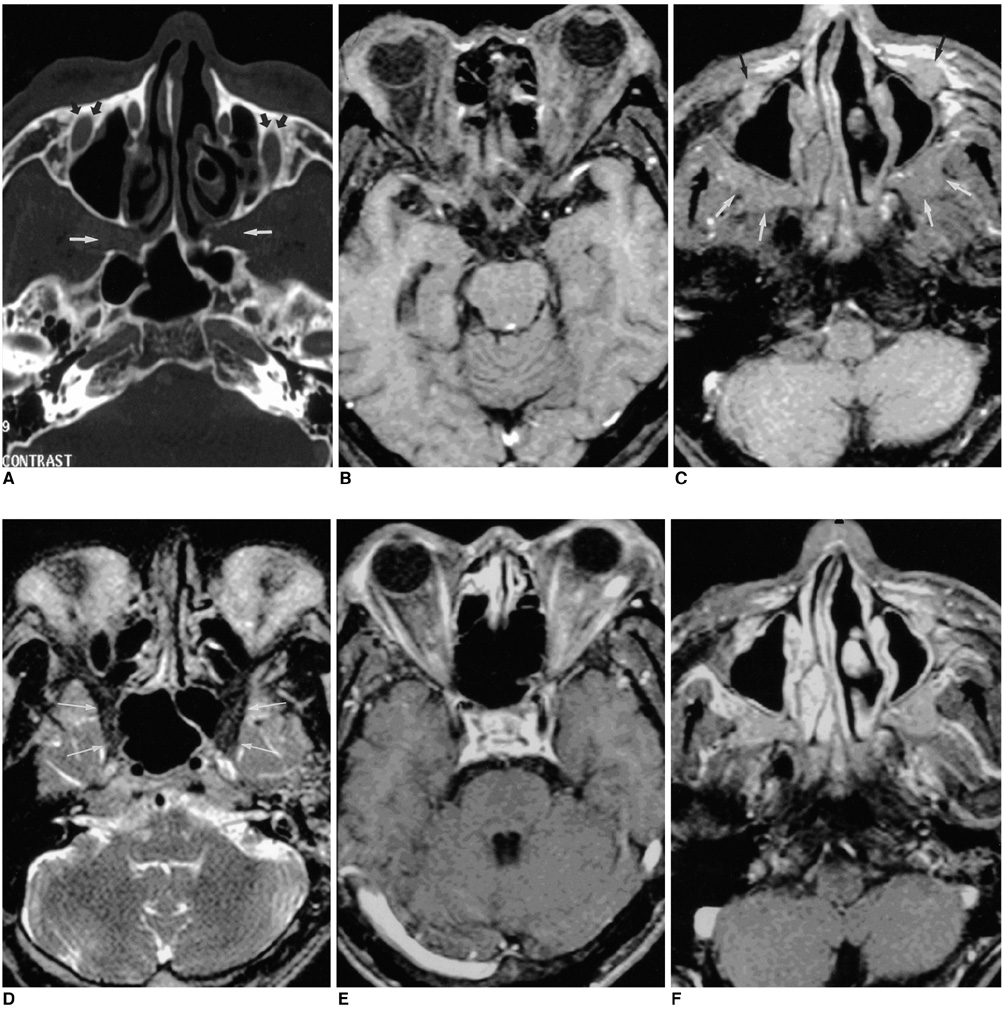
Fig. 2 Case 2. A 63-year-old man with bilateral proptosis. A. Orbital CT with bone setting shows a widening of the bilateral pterygopalatine fossae (white arrows) and the infraorbital foramina (small arrows). B, C. T1-weighted images with fat suppression show diffuse, ill-defined infiltration into the bilateral orbital fossae with involvement of the lacrimal glands and the rectus muscles. The lesions extend into the bilateral pterygopalatine and infratemporal fossae (white arrows), and infraorbital foramina (black arrows). D. T2-weighted image demonstrates that the lesions show low signal intensity. The orbital lesions extend posteriorly through the inferior orbital fissures (arrows). E, F. Postcontrast T1-weighted images reveal marked enhancement.
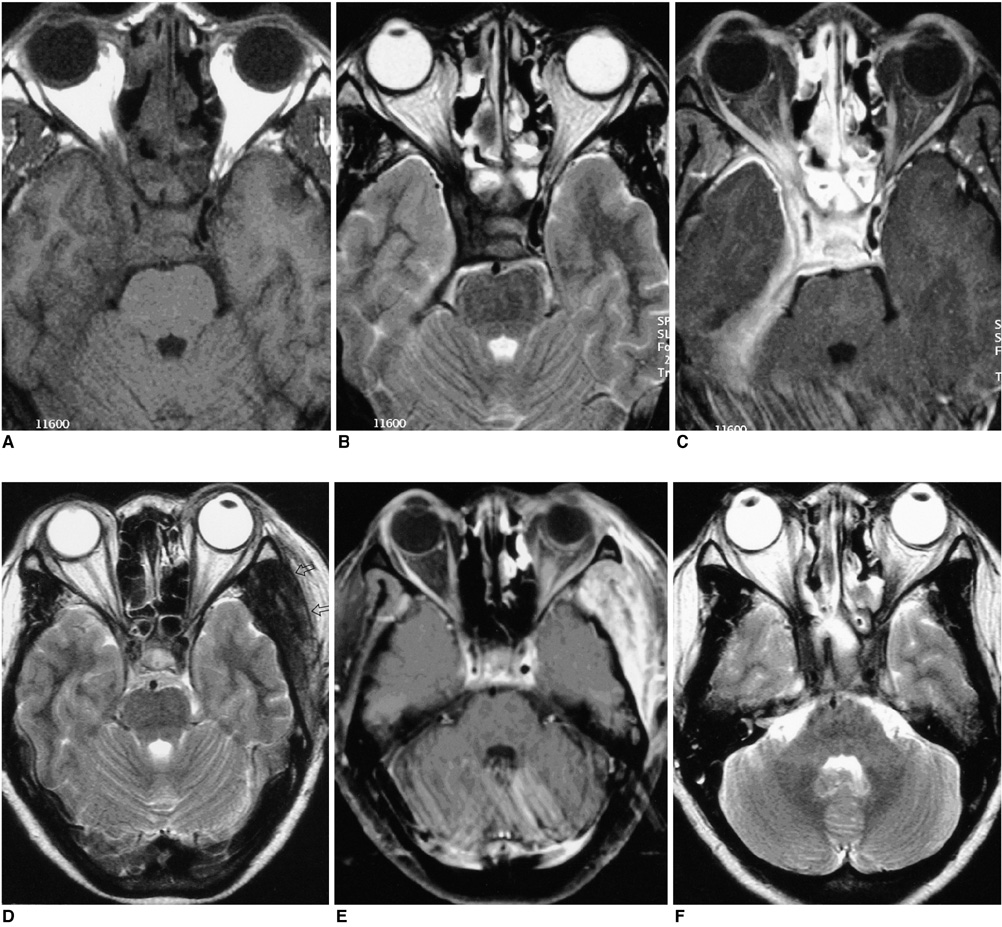
Fig. 3 Case 5. A 46-year-old man with a right proptosis and diplopia. A, B. Axial T1-weighted image (A) and T2-weighted image (B) reveal a low signal mass in the right orbital apex extending into the cavernous sinus and middle cranial fossa. Marked narrowing and encasement of the cavernous carotid artery is seen. C. Postcontrast T1-weighted image shows that the lesions are markedly enhanced. Diffuse meningeal thickening with marked enhancement is also noted. Ipsilateral medial and lateral rectus muscles are slightly thickened with some infiltration into the orbital fossa. D, E. One year later, the follow-up T2-weighted image (D) and postcontrast T1-weighted image (E) show new lesions in the left temporalis muscle (arrows), left orbital fossa and left preorbital space. The lesions show a low signal intensity on the T2-weighted image with strong enhancement. F. One year later, the follow-up T2-weighted image shows newly developed low signal lesions in the bilateral orbital fossae, orbital apices and the bilateral cavernous sinuses.
Cited by 1 articles
-
Multimodal Treatment of Skull Base Inflammatory Pseudotumor: Case Report
Sang Gun Lee, Il Young Shin, Hyung Sik Hwang, Il Choi
Brain Tumor Res Treat. 2015;3(2):122-126. doi: 10.14791/btrt.2015.3.2.122.
Reference
-
1. Bencherif B, Zouaoui A, Chedid G, Kujas M, Van Effenterre R, Marsault C. Intracranial extension of an idiopathic orbital inflammatory pseudotumor. AJNR Am J Neuroradiol. 1993. 14:181–184.2. De Jesus O, Inserni JA, Gonzalez A, Colon LE. Idiopathic orbital inflammation with intracranial extension. J Neurosurg. 1996. 85:510–513.3. Frohman LP, Kupersmith MJ, Lang J, Reede D, Bergeron RT, Aleksic S, et al. Intracranial extension and bone destruction in orbital pseudotumor. Arch Ophthalmol. 1986. 104:380–384.4. Weber AL, Romo LV, Sabates NR. Pseudotumor of the orbit. Clinical, pathologic, and radiologic evaluation. Radiol Clin North Am. 1999. 37:151–168.5. Noble SC, Chandler WF, Lloyd RV. Intracranial extension of orbital pseudotumor: a case report. Neurosurgery. 1986. 18:798–801.6. Kaye AH, Hahn JF, Craciun A, Hanson M, Berlin AJ, Tubbs RR. Intracranial extension of inflammatory pseudotumor of the orbit. J Neurosurg. 1984. 60:625–629.7. Som PM, Curtin HD. Head and neck imaging. 2003. 4th ed. St Louis: Mosby;329–330.8. Clifton AG, Borgstein RL, Moseley IF, Kendall BE, Shaw PJ. Intracranial extension of orbital pseudotumor. Clin Radiol. 1992. 45:23–26.9. Ayala AS, Fernandez Sarabia T, Cabeza Martinez B, Moya MJ, Menendez FL, Garcia PZ. Orbital pseudotumor with intracranial extension. Eur Radiol. 2000. 10:1505.10. Desai SP, Carter J, Jinkins JR. Contrast-enhanced MR imaging of Tolosa-Hunt syndrome : A case report. AJNR Am J Neuroradiol. 1991. 12:182–183.11. Goto Y, Hosokawa S, Goto I, Hirakata R, Hasuo K. Abnormality in the cavernous sinus in three patients with Tolosa-Hunt syndrome : MRI and CT findings. J Neurol Neurosurg Psychiatry. 1990. 53:231–234.12. De Arcaya AA, Cerezal L, Canga A, Polo JM, Berciano J, Pascual J. Neuroimaging diagnosis of Tolosa-Hunt syndrome MRI contribution. Headache. 1999. 39:321–325.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Classification and Treatment Efficacy of Orbital Pseudotumor
- Comparison of Orbital Pseudotumor and Lymphoma: Clinical and Radiological Findings
- Tacrolimus for Treating Orbital and Cranial Form of Idiopathic Inflammatory Pseudotumors
- Orbital wall restoring surgery with primary orbital wall fragments in blowout fracture
- Inflammatory Pseudotumor of the Extraorbital Head and Neck: CT and MR Imaging Findings
