Detectability of Various Sizes of Honeycombing Cysts in an Inflated and Fixed Lung Specimen: the Effect of CT Section Thickness
- Affiliations
-
- 1Department of Radiology, Nara Medical University, Japan.
- 2Department of Radiology, Shiga University of Medical Science, Japan. masashi@belle.shiga-med.ac.jp
- KMID: 1783168
- DOI: http://doi.org/10.3348/kjr.2005.6.1.17
Abstract
OBJECTIVE
We wanted to clarify the relationship between the visibility of air cysts on CT images, the CT slice thickness and the size of the air cysts, with contact radiographs as the gold standard, for the accurate evaluation of honeycomb cysts. MATERIALS AND METHODS: An inflated and fixed autopsied lung having idiopathic interstitial pneumonia was evaluated. The corresponding air cysts were identified on the contact radiographs of a 0.5 mm-thick-section specimen and also on the CT images of three different kinds of section thickness: 0.5, 1.0 and 2.5 mm. The maximal diameters of the air cysts were measured under a stereomicroscope. RESULTS: A total of 341 air cysts were identified on the contact radiograph, and they were then evaluated. Sixty-six percent of air cysts 1 to 2 mm in diameter were detected by 0.5 mm slice thickness CT, while only 34% and 8% were detected by 1.0 and 2.5 mm slice thickness CT, respectively. Only 28% and 22% of air cysts less than 1 mm in diameter were detected by 0.5 and 1.0 mm slice thickness CT, respectively. CT with a 2.5 mm slice thickness could not demonstrate air cysts less than 1 mm in diameter. CONCLUSION: The CT detection rate of honeycombing is significantly influenced both by the slice thickness and the size of the air cysts.
MeSH Terms
Figure
-
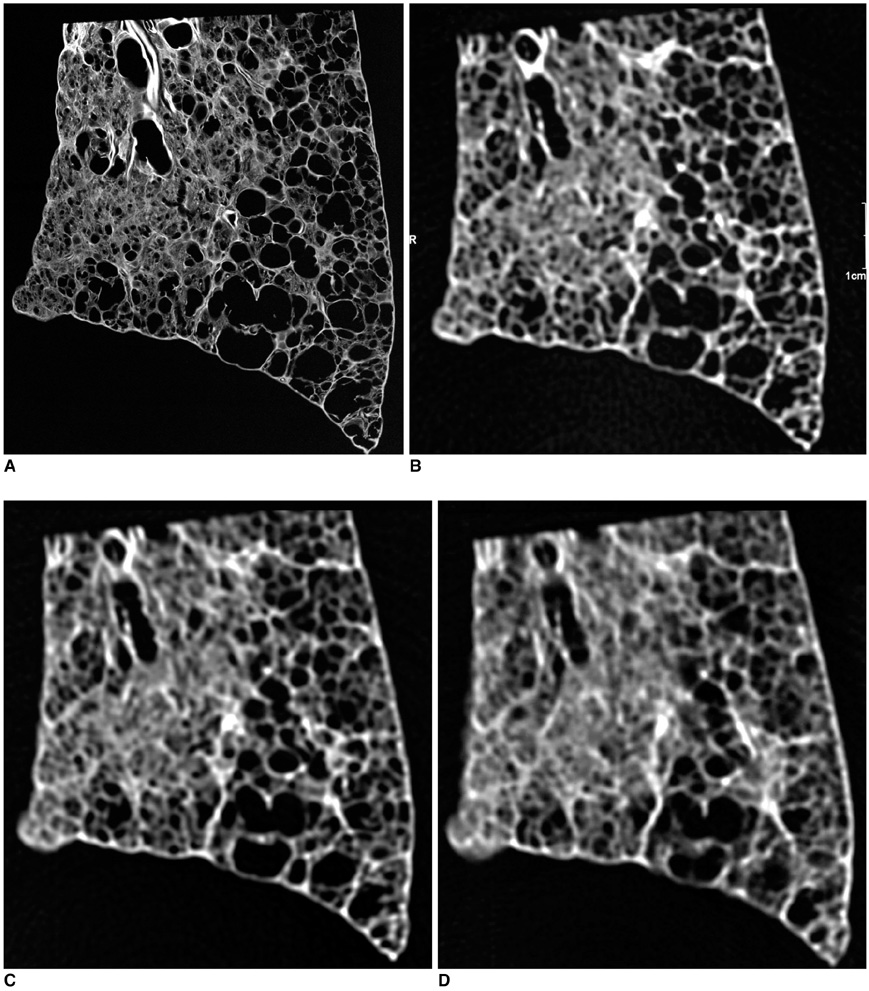
Fig. 1 A. Idiopathic pulmonary fibrosis in an 85-year-old woman. Contact radiograph of the specimen (0.5 mm thick slice). Air cysts from 1.0 to 4.0 mm in diameter were concentrated in the area of the right upper quadrant. Air cysts from 6.2 to 12.6 mm in diameter existed in the area of right lower quadrant. B. On 0.5-mm-slice-thickness CT image cysts are clearly visudized. C. On 1-mm-slice-thickness CT image, every air cyst was clearly described. The walls of the air cysts were more definite on the 0.5 mm slice thickness CT images than with 1 mm slice thickness CT images. D. On 2.5-mm-slice-thickness CT image, the margins of the small air cysts became unclear and some were recognized as reticular shadow superimposed ground grass opacity. The large air cysts were the same as on the contact radiograph.
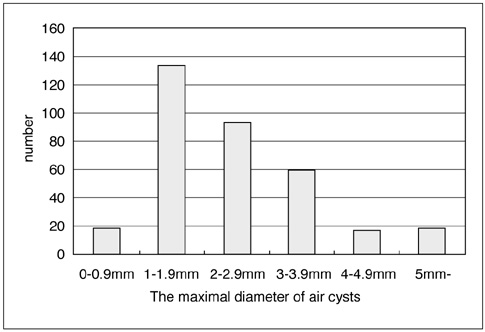
Fig. 2 The bar graph demonstrates the frequency distribution of the maximal diameter of air cysts detected on the contact radiographs.
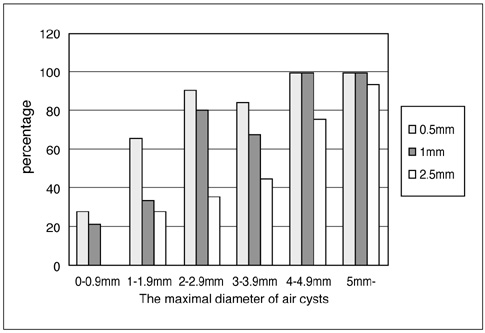
Fig. 3 The bar graph demonstrates the relationship among the ratio of detected air cysts on CT images, the size of the cysts and slice thickness.
Reference
-
1. Travis WD, King TE JR, Bateman ED, et al. American Thoracic Society/European Respiratory Society international multidisciplinary consensus classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2002. 165:277–304.2. Katzenstein AL, Myers JL. Idiopathic pulmonary fibrosis: clinical relevance of pathologic classification. Am J Respir Crit Care Med. 1998. 157:1301–1315.3. King TE JR, Costabel U, Cordier J-F, et al. American Thoracic Society. Idiopathic pulmonary fibrosis: diagnosis and treatment. Am J Respir Crit Care Med. 2000. 161:646–664.4. Itoh H, Murata K, Konishi J, Nishimura K, Kitaichi M, Izumi T. Diffuse lung disease: pathologic basis for the high-resolution computed tomography findings. J Thorac Imaging. 1993. 8:176–188.5. Nishimura K, Kitaichi M, Izumi T, Nagai S, Kanaoka M, Itoh H. Usual interstitial pneumonia: histologic correlation with high-resolution CT. Radiology. 1992. 182:337–342.6. Webb WR, Muller NL, Naidich DP. Standardized terms for high-resolution computed tomography of the lung: a proposed glossary. J Thorac Imaging. 1993. 8:167–175.7. Fraser RS, Muller NL, Colman N, Pare PD, editors. Terms for CT of the lungs. Diagnosis of diseases of the chest. 1999. 4th ed. Philadelphia: W.B. Saunders;xxxiii–xxxvi.8. Muller NL, Miller RR, Webb WR, Evans KG, Ostrow DN. Fibrosing alveolitis: CT-pathologic correlation. Radiology. 1986. 160:585–588.9. Heitzman ER. The lung: radiologic-pathologic correlations. 1984. 2nd ed. St. Louis: Mosby;4–12.10. Nakata H, Kimoto T, Nakayama T, Kido M, Miyazaki N, Harada S. Diffuse peripheral lung disease: evaluation by high-resolution computed tomography. Radiology. 1985. 157:181–185.11. Muller NL, Staples CA, Miller RR, Vedal S, Thurlbeck WM, Ostrow DN. Disease activity in idiopathic pulmonary fibrosis: CT and pathologic correlation. Radiology. 1987. 165:731–734.12. Murata K, Khan A, Rojas KA, Herman PG. Optimization of computed tomography technique to demonstrate the fine structure of the lung. Invest Radiol. 1988. 23:170–175.13. Noma S, Kubo T, Kuroda Y, et al. Definition of honeycombing on HRCT and microscopic honeycombing. Jpn J Clin Radiol. 1999. 44:73–77.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Detection of the Anatomic Structure and Pathology in Animal Lung Specimens: Comparison of Micro CT and Multi-Detector Row CT
- Cystic Lung Disease: a Comparison of C ystic Size, as Seen on Expira tory and Inspiratory HRCT Scans
- A study of Parameters in Spiral CT Volumetry Using Balloon Phantoms
- Ultra-Low-Dose MDCT of the Chest: Influence on Automated Lung Nodule Detection
- Hematogeneous pulmonary metastasis: an experimental study by using VX-2 carcinoma in rabbit
