Impact of Combined Acute Rejection on BK Virus-Associated Nephropathy in Kidney Transplantation
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea.
- 2Transplantation Center, Seoul National University Hospital, Seoul, Korea. jcyjs@dreamwiz.com
- 3Transplantation Research Institute, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 1779409
- DOI: http://doi.org/10.3346/jkms.2013.28.12.1711
Abstract
- BK virus-associated nephropathy (BKVAN) is one of the major causes of allograft dysfunction in kidney transplant (KT) patients. We compared BKVAN combined with acute rejection (BKVAN/AR) with BKVAN alone in KT patients. We retrospectively analyzed biopsy-proven BKVAN in KT patients from 2000 to 2011 at Seoul National University Hospital. Among 414 biopsies from 951 patients, biopsy-proven BKVAN was found in 14 patients. Nine patients had BKVAN alone, while 5 patients had both BKVAN and acute cellular rejection. BKVAN in the BKVAN alone group was detected later than in BKVAN/AR group (21.77 vs 6.39 months after transplantation, P=0.03). Serum creatinine at diagnosis was similar (2.09 vs 2.00 mg/dL). Histological grade was more advanced in the BKVAN/AR group (P=0.034). Serum load of BKV, dose of immunosuppressants, and tacrolimus level showed a higher tendency in the BKVAN alone group; however it was not statistically significant. After anti-rejection therapy, immunosuppression was reduced in the BKVAN/AR group. Renal functional deterioration over 1 yr after BKVAN diagnosis was similar between the two groups (P=0.665). These findings suggest that the prognosis of BKVAN/AR after anti-rejection therapy followed by anti-BKV therapy might be similar to that of BKVAN alone after anti-BKV therapy.
MeSH Terms
-
Acute Disease
Adult
Antiviral Agents/therapeutic use
BK Virus/*physiology
Creatinine/blood
Female
*Graft Rejection/diagnosis/virology
Humans
Immunosuppressive Agents/administration & dosage
Kidney/*virology
Kidney Diseases/pathology/surgery/*virology
*Kidney Transplantation
Male
Middle Aged
Polyomavirus Infections/drug therapy/*etiology/pathology
Retrospective Studies
Tacrolimus/administration & dosage
Time Factors
Transplantation, Homologous/adverse effects
Tumor Virus Infections/drug therapy/*etiology/pathology
Antiviral Agents
Creatinine
Immunosuppressive Agents
Tacrolimus
Figure
-
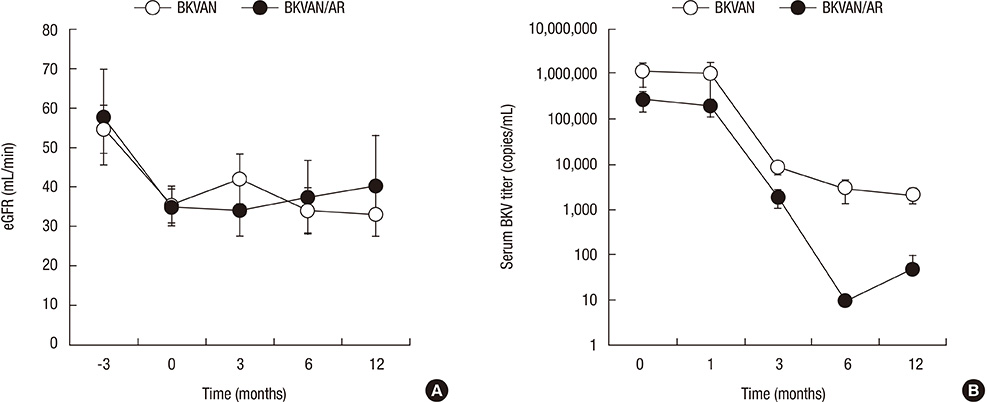
Fig. 1 Courses of renal function and BK viral load in BK virus nephropathy with or without acute rejection. (A) After abrupt reduction of renal function before treatment of BKVAN, renal function was stabilized over 1 yr after BKVAN. There was no significant difference in renal function in 1 yr after diagnosis of BKVAN between BKVAN alone and BKVAN combined with acute rejection. Zero time indicated diagnosis time for BKVAN. Each value was expressed as mean with standard error. P > 0.05 at all time points. (B) BK viral load had decreased after treatment of BKVAN in both groups. Although BK viral loads in the BKV alone group were higher than those in the BKVAN combined with acute rejection group, the differences were not statistically significant (P > 0.05 at all time-points). Zero time indicated diagnosis time for BKVAN. Each value was expressed as mean with standard error. eGFR, estimated glomerular filtration rate. BKVAN, BKVAN alone; BKVAN/AR, BKVAN combined with acute rejection.
Cited by 1 articles
-
Bortezomib Treatment for Refractory Antibody-Mediated Rejection Superimposed with BK Virus-Associated Nephropathy during the Progression of Recurrent C3 Glomerulonephritis
Wonseok Do, Jong-Hak Lee, Kyung Joo Kim, Man-Hoon Han, Hee-Yeon Jung, Ji-Young Choi, Sun-Hee Park, Yong-Lim Kim, Chan-Duck Kim, Jang-Hee Cho, Youngae Yang, Minjung Kim, Inryang Hwang, Kyu Yeun Kim, Taehoon Yim, Yong-Jin Kim
J Korean Soc Transplant. 2018;32(3):57-62. doi: 10.4285/jkstn.2018.32.3.57.
Reference
-
1. Hirsch HH, Knowles W, Dickenmann M, Passweg J, Klimkait T, Mihatsch MJ, Steiger J. Prospective study of polyomavirus type BK replication and nephropathy in renal-transplant recipients. New Engl J Med. 2002; 347:488–496.2. Hirsch HH, Brennan DC, Drachenberg CB, Ginevri F, Gordon J, Limaye AP, Mihatsch MJ, Nickeleit V, Ramos E, Randhawa P, et al. Polyomavirus-associated nephropathy in renal transplantation: interdisciplinary analyses and recommendations. Transplantation. 2005; 79:1277–1286.3. Drachenberg CB, Hirsch HH, Ramos E, Papadimitriou JC. Polyomavirus disease in renal transplantation: review of pathological findings and diagnostic methods. Hum Pathol. 2005; 36:1245–1255.4. McGilvray ID, Lajoie G, Humar A, Cattral MS. Polyomavirus infection and acute vascular rejection in a kidney allograft: coincidence or mimicry? Am J Transplant. 2003; 3:501–504.5. Ramos E, Drachenberg CB, Wali R, Hirsch HH. The decade of polyomavirus BK-associated nephropathy: state of affairs. Transplantation. 2009; 87:621–630.6. Sánchez Fructuoso AI, Calvo N, Perez-Flores I, Valero R, Rodríguez-Sánchez B, García de Viedma D, Muñoz P, Barrientos A. Mammalian target of rapamycin signal inhibitors could play a role in the treatment of BK polyomavirus nephritis in renal allograft recipients. Transpl Infect Dis. 2011; 13:584–591.7. Ito Y, Nishi S, Imai N, Yoshita K, Saito K, Nakagawa Y, Takahashi K, Narita I. The case of BK virus infection in which it was difficult to differentiate from acute rejection. Clin Transplant. 2011; 25:44–48.8. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation: Modification of Diet in Renal Disease Study Group. Ann Intern Med. 1999; 130:461–470.9. Masutani K, Shapiro R, Basu A, Tan H, Wijkstrom M, Randhawa P. The Banff 2009 Working Proposal for polyomavirus nephropathy: a critical evaluation of its utility as a determinant of clinical outcome. Am J Transplant. 2012; 12:907–918.10. Solez K, Colvin RB, Racusen LC, Haas M, Sis B, Mengel M, Halloran PF, Baldwin W, Banfi G, Collins AB, et al. Banff 07 classification of renal allograft pathology: updates and future directions. Am J Transplant. 2008; 8:753–760.11. Hirsch HH, Randhawa P. AST Infectious Diseases Community of Practice. BK virus in solid organ transplant recipients. Am J Transplant. 2009; 9:S136–S146.12. Egli A, Köhli S, Dickenmann M, Hirsch HH. Inhibition of polyomavirus BK-specific T-cell responses by immunosuppressive drugs. Transplantation. 2009; 88:1161–1168.13. Araki K, Turner AP, Shaffer VO, Ganqappa S, Keller SA, Bachmann MF, Larsen CP, Ahmed R. mTOR regulates memory CD8 T-cell differentiation. Nature. 2009; 460:108–112.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of BK Virus Nephropathy with Strong C4d Deposition in a Renal Allograft Recipient
- Treatment of Presumptive BK Nephropathy with Ciprofloxain in Kidney Transplant Recipients: Three Case Reports
- Long-term prognosis of BK virus-associated nephropathy in kidney transplant recipients
- Leflunomide Treatment in BK Virus Associated Nephropathy after Renal Transplantation
- Effect of High Dose Intravenous Immunoglobulins on the Treatment of Antibody Mediated Humoral Rejection and BK Virus Infection in Renal Transplant Recipients
