J Korean Med Sci.
2011 Jan;26(1):143-145. 10.3346/jkms.2011.26.1.143.
A Case of Campomelic Dysplasia without Sex Reversal
- Affiliations
-
- 1Department of Pediatrics, Division of Neonatology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. arkim@amc.seoul.kr
- 2Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 3Department of Medical Genetics Clinic and Laboratory, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 1777990
- DOI: http://doi.org/10.3346/jkms.2011.26.1.143
Abstract
- Campomelic dysplasia (CD; OMIM #114290), a rare form of congenital short-limbed dwarfism, is due to mutations in SOX9, a member of the SOX (SRY-related HMG box) gene family. Multiparous mother at 38 weeks' gestation delivered a 3,272 g baby boy with characteristic phenotypes including bowing of the lower limbs, a narrow thoracic cage, 11 pairs of ribs, hypoplastic scapulae, macrocephaly, flattened supraorbital ridges and nasal bridge, cleft palate, and micrognathia. He underwent a tracheostomy at the age of three months for severe laryngomalacia after a number of repeated hospitalizations due to respiratory problems and died at the age of four months from progressive respiratory failure. He was diagnosed as having CD based on a novel frameshift mutation (p.Gln458ArgfsX12) in the SOX9 gene, the mutation which has not yet been reported in Korea.
Keyword
MeSH Terms
Figure
-
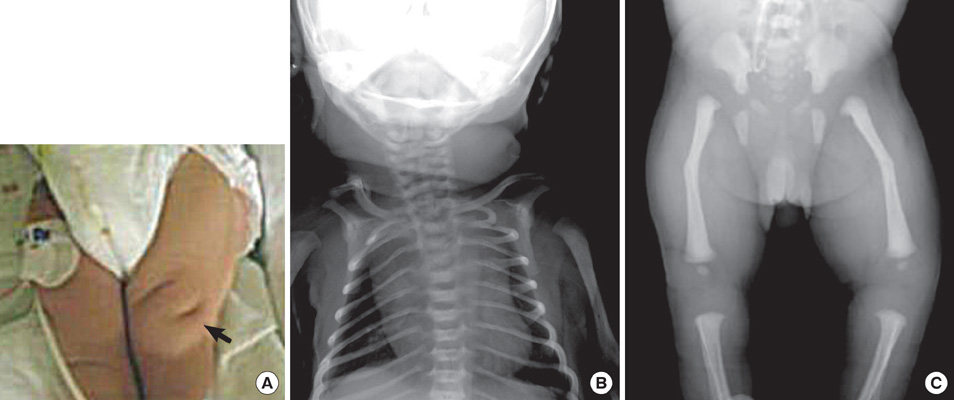
Fig. 1 Clinical features of a campomelic dysplasia patient. (A) Pretibial skin dimple (arrow) on the left thigh. (B) Chest radiography shows a bell-shaped, narrow thoracic cage, hypoplastic scapulae and mild T-L scoliosis. (C) Radiograph of bilateral legs shows anterolateral femoral bowing and short fibulae.

Fig. 2 DNA sequencing of the SOX9 gene. (A) Normal control. (B) Patient. A novel frameshift mutation (p.Gln458ArgfsX12) was noticed at nucleotide 1372 (circle).
Reference
-
1. Wagner T, Wirth J, Meyer J, Zabel B, Held M, Zimmer J, Pasantes J, Bricarelli FD, Keutel J, Hustert E, Wolf U, Tommerup N, Schempp W, Scherer G. Autosomal sex reversal and campomelic dysplasia are caused by mutations in and around the SRY-related gene SOX9. Cell. 1994. 79:1111–1120.2. Kwok C, Weller PA, Guioli S, Foster JW, Mansour S, Zuffardi O, Punnett HH, Dominguez-Steglich MA, Brook JD, Young ID, Goodfellow PN, Schafer AJ. Mutations in SOX9, the gene responsible for Campomelic dysplasia and autosomal sex reversal. Am J Hum Genet. 1995. 57:1028–1036.3. Stoll C, Dott B, Roth MP, Alembik Y. Birth prevalence rates of skeletal dysplasias. Clin Genet. 1989. 35:88–92.4. Maroteaux P, Spranger J, Opitz JM, Kucera J, Lowry RB, Schimke RN, Kagan SM. The campomelic syndrome. Presse Med. 1971. 79:1157–1162.5. Mansour S, Hall CM, Pembrey ME, Young ID. A clinical and genetic study of campomelic dysplasia. J Med Genet. 1995. 32:415–420.6. Horton WA, Hecht JT. Behrman RE, Kliegman RM, Jenson HB, editors. The skeletal dysplasia. Textbook of Pediatrics. 2000. 16th ed. Philadelphia: WB Saunders Co;2113–2132.7. Argaman Z, Hammerman CA, Kaplan M, Schimmel M, Rabinovich R, Tunnessen WW Jr. Picture of the month. Campomelic dysplasia. Am J Dis Child. 1993. 147:205–206.8. Hall BD, Spranger JW. Campomelic dysplasia. Further elucidation of a distinct entity. Am J Dis Child. 1980. 134:285–289.9. Jones KL. Smith's Recognizable Patterns of Human Malformation. 1997. 5th ed. Philadelphia: WB Saunders Co;344–345.10. Foster JW, Dominguez-Steglich MA, Guioli S, Kowk C, Weller PA, Stevanović M, Weissenbach J, Mansour S, Young ID, Goodfellow PN, Brook JD, Schafer AJ. Campomelic dysplasia and autosomal sex reversal caused by mutations in an SRY-related gene. Nature. 1994. 372:525–530.11. Offiah AC, Mansour S, McDowall S, Tolmie J, Sim P, Hall CM. Surviving campomelic dysplasia has the radiological features of the previously reported ischio-pubic-patella syndrome. J Med Genet. 2002. 39:e50.12. Hill-Harfe KL, Kaplan L, Stalker HJ, Zori RT, Pop R, Scherer G, Wallace MR. Fine mapping of chromosome 17 translocation breakpoints > or = 900 Kb upstream of SOX9 in acampomelic campomelic dysplasia and a mild, familial skeletal dysplasia. Am J Hum Genet. 2005. 76:663–671.13. Bianchi ME, Beltrame M. Flexing DNA: HMG-box proteins and their partners. Am J Hum Genet. 1998. 63:1573–1577.14. McDowall S, Argentaro A, Ranganathan S, Weller P, Mertin S, Mansour S, Tolmie J, Harley V. Functional and structural studies of wild type SOX9 and mutations causing campomelic dysplasia. J Biol Chem. 1999. 274:24023–24030.15. Bell DM, Leung KK, Wheatley SC, Ng Lj, Zhou S, Ling KW, Sham MH, Koopman P, Tam PP, Cheah KS. SOX9 directly regulates the type-II collagen gene. Nat Genet. 1997. 16:174–178.16. De Santa Barbara P, Bonneaud N, Boizet B, Desclozeaux M, Moniot B, Sudbeck P, Scherer G, Poulat F, Berta P. Direct interaction of SRY-related protein SOX9 and steroidogenic factor 1 regulates transcription of the human anti-Müllerian hormone gene. Mol Cell Biol. 1998. 18:6653–6665.17. Cameron FJ, Sinclair AH. Mutations in SRY and SOX9: testis-determining genes. Hum Mutat. 1997. 9:388–395.18. Bernard P, Tang P, Liu S, Dewing P, Harley VR, Vilain E. Dimerization of SOX9 is required for chondrogenesis, but not for sex determination. Hum Mol Genet. 2003. 12:1755–1765.19. Chung CQ, Bae HY, Kim DR, Park YH, Chung HS. A case of multiple congenital anomaly. Korean J Obstet Gynecol. 1992. 35:1407–1413.20. Kim SK, Kim HC, Shin SJ, Lee MW, Lee YM, Cho JH, Choi YJ, Kwon KW. A case of fetal skeletal anomaly of Campomelic syndrome. Korean J Obstet Gynecol. 2000. 43:311–314.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of fetal skelectal anomaly of Campomelic syndrome
- Campomelic Dysplasia with Sex Reversal Harboring a Novel Frameshift Mutation
- A Korean Girl with Campomelic Dysplasia caused by a Novel Nonsense Mutation within the SOX9 Gene
- Prevalence of Intestinal Metaplasia, Dysplasia and Helicobacter pylori Infection by Aging
- A Case of Retinal Dysplasia with PHPV
