Precordial ST-Segment Elevation in Acute Right Ventricular Myocardial Infarction
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Gangneung Asan Hospital, Gangneung, Korea. bovio@naver.com
- KMID: 1776351
- DOI: http://doi.org/10.4070/kcj.2008.38.9.495
Abstract
- It is rare to observe ST-segment elevations in the precordial leads that are caused by an occlusion of the right coronary artery and/or its branches. We report here on two cases of acute occlusion of the right coronary artery or its branches that caused acute right ventricular myocardial infarction with ST-segment elevations in the anterior precordial leads. These cases should remind us that the presence of diffuse ST-segment elevations in the precordial leads could be due to acute occlusion of the right coronary artery.
Figure
-
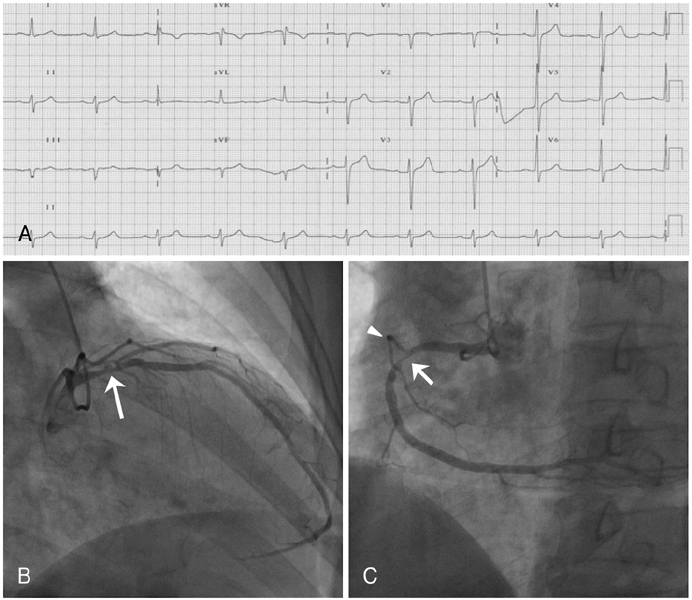
Fig. 1 Electrocardiography (ECG) and diagnostic coronary angiography findings on admission. A: the electrocardiography on admission showed normal sinus rhythm and no significant ischemic ST-segment deviations. B and C: the initial coronary angiography showed significant luminal narrowing at the proximal segments of the left anterior descending artery and the right coronary artery (arrows), and an open right ventricular side branch with normal distal flow (arrowhead).
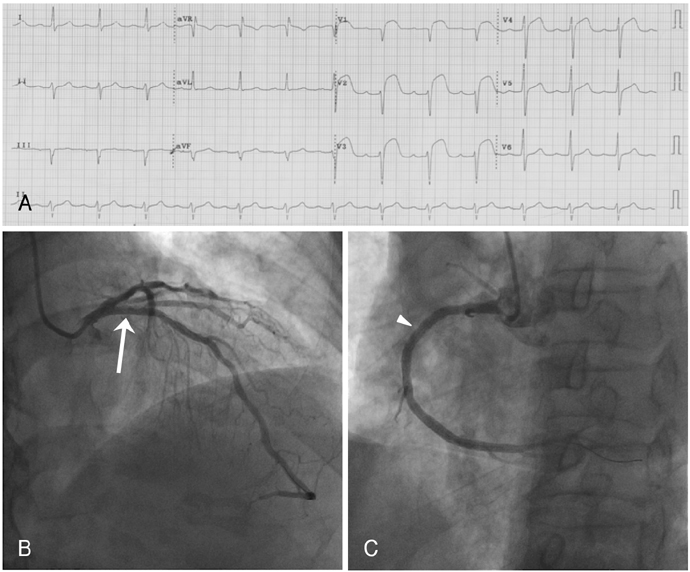
Fig. 2 Electrocardiography (ECG) and coronary angiography findings after percutaneous coronary intervention (PCI). A: the electrocardiography immediately after percutaneous coronary intervention showed marked ST-segment elevations in the precordial leads. B and C: repeated coronary angiography showed that the left anterior descending artery and the stented area were open with normal coronary flow (arrow), but the right ventricular branch was stent-jailed (arrowhead).
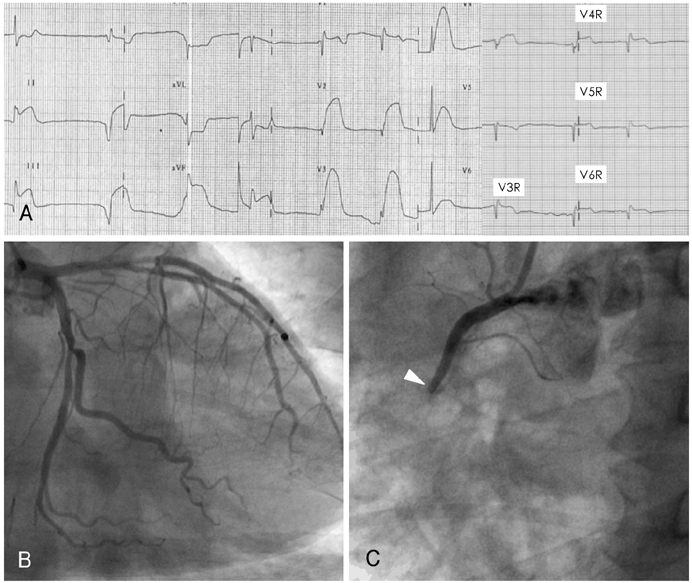
Fig. 3 Electrocardiography (ECG) and diagnostic coronary angiography findings on admission. A: the initial electrocardiography on admission showed atrio-ventricular block and marked ST-segment elevations in both the inferior and precordial leads and 1 mm ST-segment elevations from V4R to V6R. B: the initial coronary angiography revealed no significant luminal narrowing of the left coronary arteries. C: note the total occlusion at the proximal segment of the right coronary artery with TIMI 0 flow (arrowhead). TIMI: Thrombolysis In Myocardial Infarction.
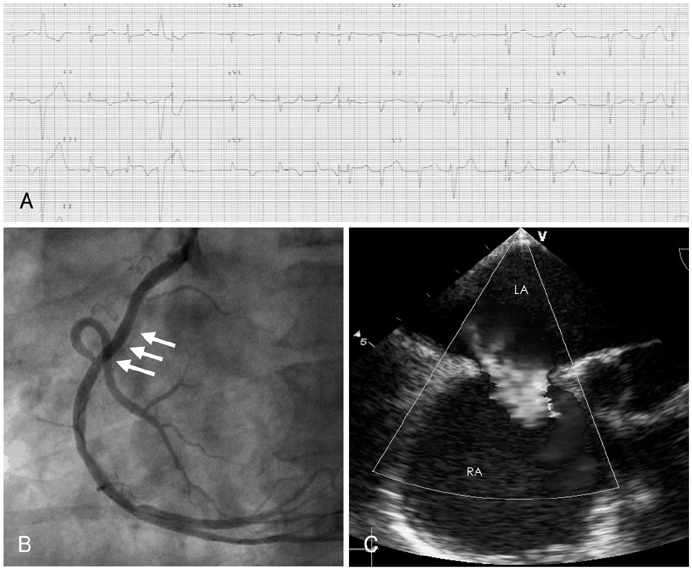
Fig. 4 Electrocardiography (ECG), coronary angiography, and transesophagreal echocardiography (TEE) findings after percutaneous coronary intervention (PCI). A: the electrocardiography after percutaneous coronary intervention showed resolution of the ST-segment elevation in the precordial leads. B: the coronary angiography, following percutaneous coronary intervention, showed a good appearance with TIMI 3 flow (arrows). C: the transesophageal echocardiography revealed the secundum type of atrial septal defect with left to right shunt. LA: left atrium, RA: right atrium, TIMI: Thrombolysis In Myocardial Infarction.
Reference
-
1. Porter A, Herz I, Strasberg B. Isolated right ventricular infarction presenting as anterior wall myocardial infarction on electrocardiography. Clin Cardiol. 1997. 20:971–973.2. Saw J, Amin H, Kiess M. Right ventricular ischemia mimicking acute anterior myocardial infarction. Can J Cardiol. 1999. 15:1143–1146.3. Khan ZU, Chou TC. Right ventricular infarction mimicking acute anteroseptal left ventricular infarction. Am Heart J. 1996. 132:1089–1093.4. Lew AS, Maddhai J, Shah PK, et al. Factors that determine the direction and magnitude of precordial ST-segment deviations during inferior wall acute myocardial infarction. Am J Cardiol. 1985. 55:883–888.5. Geft I, Shah P, Rodriguez L, et al. ST elevations in leads V1 to V5 may be caused by right coronary artery occlusion and acute right ventricular infarction. Am J Cardiol. 1984. 53:991–996.6. Eskola MJ, Nikus KC, Niemela KO, Sclarovsky S. How to use ECG for decision support in the catheterization laboratory: cases with inferior ST elevation myocardial infarction. J Electrocardiol. 2004. 37:257–266.7. Eskola MJ, Kosonen P, Sclarovsky S, Vikman S, Nikus KC. The ECG pattern of isolated right ventricular infarction during percutaneous coronary intervention. Ann Noninvasive Electrocardiol. 2007. 12:83–87.8. van der Bolt CL, Vermeersch PH, Plokker HW. Isolated acute occlusion of a large right ventricular branch of the right coronary artery following coronary balloon angioplasty: the only true 'model' to study ECG changes in acute, isolated right ventricular infarction. Eur J Heart. 1996. 17:247–250.9. Kim MS, Han JK, Lee SE, et al. Cases of right ventricular myocardial infarction in patients with an absent or hypoplastic right coronary artery. Korean Cir J. 2007. 37:84–86.10. Chia BL, Yip JW, Tan HC, Lim YT. Usefulness of ST elevation II/III ratio and ST deviation in lead I for identifying the culprit artery in inferior wall acute myocardial infarction. Am J Cardiol. 2000. 86:341–343.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Myocardial Infarction by Right Coronary Artery Occlusion Presenting as Precordial ST Elevation on Electrocardiography
- ST segment
- The Prognostic Significance of Maximal Precordial ST-Segment Depression in Patients with Acute Inferior Myocardial Infarction
- The Significance of the Precordial ST: segment Depression in Acute (V1- V3) Inferior Myocardial Infarction
- Clinical Significance of Precordial ST Segment Depression in Acute Inferior Myocardial Infarction
