A Case of Malignant Pericardial Mesothelioma With Constrictive Pericarditis Physiology Misdiagnosed as Pericardial Metastatic Cancer
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Inha University College of Medicine, Incheon, Korea. kdhmd@inha.ac.kr
- KMID: 1776193
- DOI: http://doi.org/10.4070/kcj.2011.41.6.338
Abstract
- Malignant pericardial mesothelioma is a rare and progressive cardiac tumor. There is no established standard treatment and the prognosis is poor. Most patients were retrospectively diagnosed from surgery or autopsy due to absence of specific clinical manifestation. Most patients with pericardial mesothelioma have demonstrated constrictive physiology on echocardiography or cardiac catheterization. Therefore, pericardial mesothelioma was often misdiagnosed as other causes of constrictive pericarditis. We report a case of primary pericardial mesothelioma misdiagnosed as pericardial metastasis of unknown origin.
Keyword
MeSH Terms
Figure
-

Fig. 1 A: transthoracic echocardiography demonstrated pericardial thickening (arrow) without pericardial effusion on the short axis view. B: Doppler echocardiography demonstrated difference in peak early diastolic velocity between inspiration (blue 1) and expiration (blue 2). LV: left ventricle, RV: right ventricle.
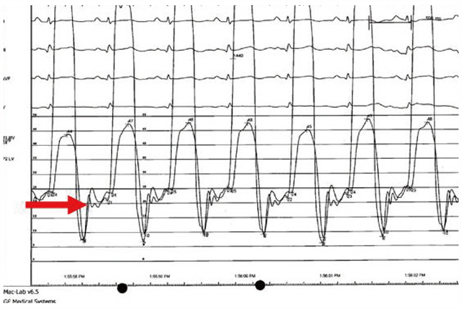
Fig. 2 Cardiac catheterization demonstrated rapid rising of early diastolic pressures and abrupt equalization in both ventricles (red arrow), namely the dip and plateau pattern. Diastolic pressures of the left and right ventricles are demonstrated.
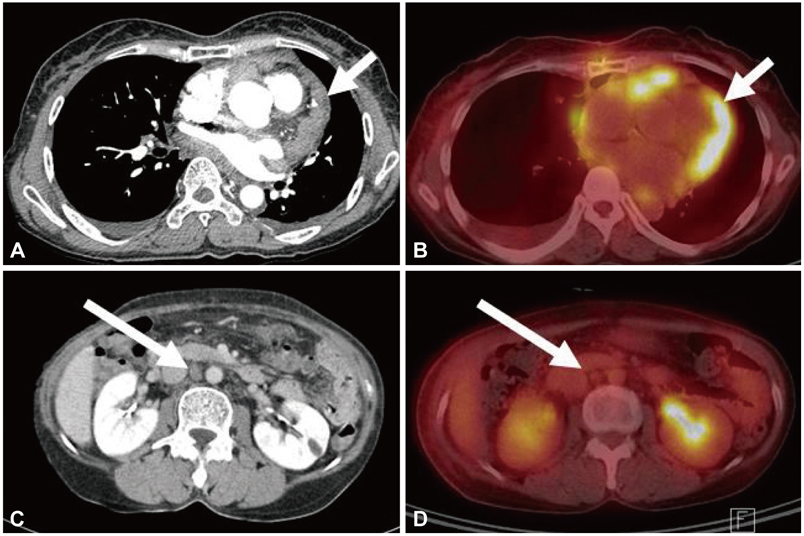
Fig. 3 A: chest CT demonstrated thickened pericardium with multiple pericardial nodules (arrow) and bilateral pleural effusion. B: PET-CT demonstrated significant FDG uptake in the pericardium (arrow) with a maximal standardized uptake value of 6.18. C: abdominal CT demonstrated a 1.4 cm sized aortocarval lymphadenopathy (arrow). D: PET-CT demonstrated no significant FDG uptake in the aortocarval lymph node (arrow). PET: positron emission tomography, FDG: fluorodeoxyglucose.
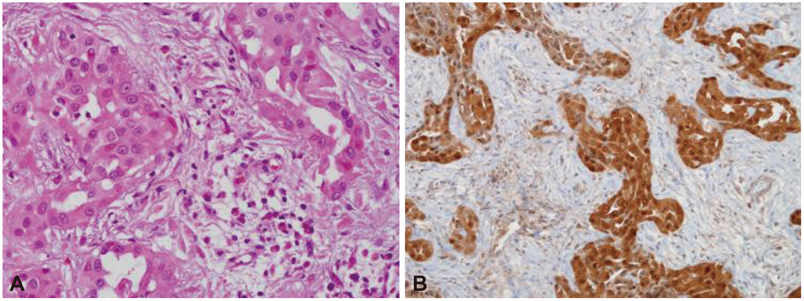
Fig. 4 A: microscopic examination showed abundant pleomorphic malignant cells with epithelial appearance (H&E stain, ×400). B: positive immunochemical staining with calretinin.
Reference
-
1. Kralstein J, Frishman W. Malignant pericardial diseases: diagnosis and treatment. Am Heart J. 1987. 113:785–790.2. Gossinger HD, Siostrznek P, Zangeneh M, et al. Magnetic resonance imaging findings in a patient with pericardial mesothelioma. Am Heart J. 1988. 115:1321–1322.3. Suman S, Schofield P, Large S. Primary pericardial mesothelioma presenting as pericardial constriction: case report. Heart. 2004. 90:e4.4. Ha CB, Huh JY, Shin YW, Shin YK. Doppler flow patterns of constrictive pericarditis. Korean Circ J. 1989. 19:47–54.5. Cherian G, Habashy A, Uthaman B, Cherian J, Salama A, Anim J. Detection and follow-up of mediastinal lymph node enlargement in tuberculous pericardial effusions using computed tomography. Am J Med. 2003. 114:319–322.6. Ha JW, Ko YG, Choi BW. Images in cardiology: delayed hyperenhancement of the pericardium by magnetic resonance imaging as a marker of pericardial inflammation in a patient with tuberculous effusive constrictive pericarditis. Heart. 2006. 92:494.7. Kaminaga T, Takeshita T, Kimura I. Role of magnetic resonance imaging for evaluation of tumors in the cardiac region. Eur Radiol. 2003. 13:Suppl 6. L1–L10.8. Flores RM, Akhurst T, Gonen M, et al. Positron emission tomography defines metastatic disease but not locoregional disease in patients with malignant pleural mesothelioma. J Thorac Cardiovasc Surg. 2003. 126:11–16.9. Ost P, Rottey S, Smeets P, Boterberg T, Stragier B, Goethals I. F-18 fluorodeoxyglucose PET/CT scanning in the diagnostic work-up of a primary pericardial mesothelioma. J Thorac Imaging. 2008. 23:35–38.10. Lagrotteria DD, Tsang B, Elavathil LJ, Tomlinson CW. A case of primary malignant pericardial mesothelioma. Can J Cardiol. 2005. 21:185–187.11. Kaul TK, Fields BJ, Kahn DR. Primary malignant pericardial mesothelioma: a case report and review. J Cardiovasc Surg (Torino). 1994. 35:261–267.12. Ceresoli GL, Zucali PA, Favaretto AG, et al. Phase II study of pemetrexed plus carboplatin in malignant pleural mesothelioma. J Clin Oncol. 2006. 24:1443–1448.13. Kindler HL, Herndon JE, Zhang C, Green MR. Irinotecan for malignant mesothelioma A phase II trial by the Cancer and Leukemia Group B. Lung Cancer. 2005. 48:423–428.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Malignant Pericardial Mesothelioma Misdiagnosed as Constrictive Pericarditis
- A case of malignant pericardial mesothelioma misdiagnosed as tuberculosis pericarditis
- A Case of Constrictive Pericarditis with Localized Pericardial Effusion Simulating a Cystic Mass
- Primary Malignant Pericardial Mesothelioma Presenting as Acute Pericarditis
- Surgical Experience of Pericardial Mesothelioma: 2 Cases
