Korean J Gastroenterol.
2012 Jan;59(1):48-52. 10.4166/kjg.2012.59.1.48.
Liver Cirrhosis Due to Autoimmune Hepatitis Combined with Systemic Sclerosis
- Affiliations
-
- 1Department of Internal Medicine, Soon Chun Hyang University College of Medicine, Seoul, Korea. jeongsw@schmc.ac.kr
- 2Department of Pathology, Soon Chun Hyang University College of Medicine, Seoul, Korea.
- KMID: 1775833
- DOI: http://doi.org/10.4166/kjg.2012.59.1.48
Abstract
- Systemic sclerosis (SSc) is a chronic systemic disease that affects the skin, lungs, heart, gastrointestinal tract, kidneys, and musculoskeletal system. Although up to 90% of patients with scleroderma have been estimated to have gastrointestinal involvement, liver disease has been reported only rarely. A 51-year-old woman was hospitalized due to esophageal variceal bleeding. Her serum was positive for anti-nuclear antibody and anti-centromere antibody. Sclerodactyly was noted on both hands, and she had recently developed Raynaud's syndrome. Punch biopsy of the hand showed hyperkeratosis, regular acanthosis, and increased basal pigmentation in the epidermis, and thick pale collagenous bundles in the dermis. Liver biopsy showed chronic active hepatitis with bridging fibrosis. Consequently, she was diagnosed with liver cirrhosis due to autoimmune hepatitis (AIH) combined with SSc. AIH had subsided after administration of prednisolone at 40 mg per day. She received 5-10 mg/day of prednisolone as an outpatient, and her condition has remained stable. Patients with either AIH or SSc should be monitored for further development of concurrent autoimmune diseases. The early diagnosis of AIH combined with SSc will be helpful in achieving optimal management.
MeSH Terms
-
Anti-Inflammatory Agents/therapeutic use
Antibodies, Antinuclear/blood
Esophageal and Gastric Varices
Female
Gastrointestinal Hemorrhage
Hepatitis, Autoimmune/complications/*diagnosis/drug therapy
Humans
Liver Cirrhosis/*diagnosis/etiology/pathology
Middle Aged
Prednisolone/therapeutic use
Raynaud Disease/diagnosis
Scleroderma, Systemic/complications/*diagnosis
Skin/pathology
Figure
-

Fig. 1 Skin manifestations and biopsy. (A) Sclerodactyly development at the tips of the fingers, skin indurations, and fixed flexion contractures at the proximal interphalangeal joints. (B) Section of the skin biopsy specimen showing collagen bundles of the reticular dermis appear to be thickened, hypocellular and deeply eosinophilic (H&E, ×200).
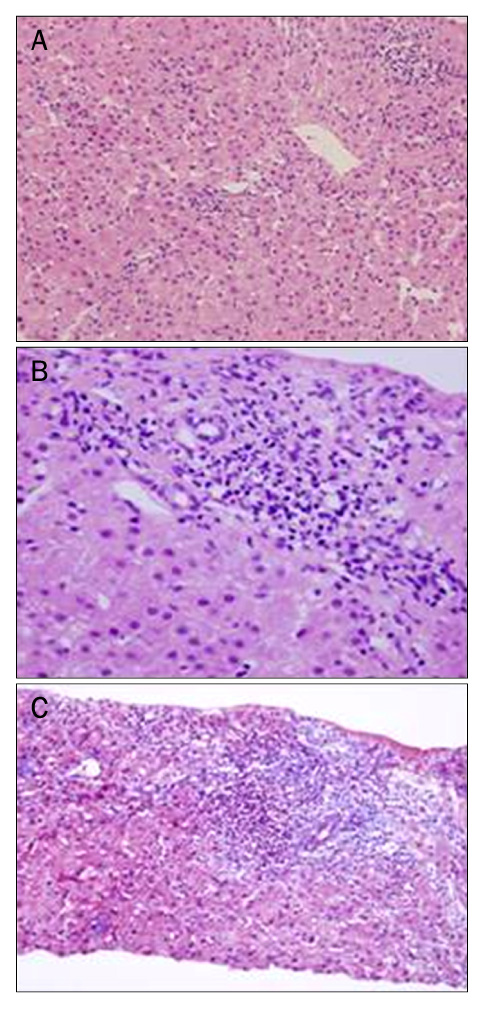
Fig. 2 Liver biopsy. (A) Multiple drop out of hepatocytes replaced by lymphoid cells and acidophilic bodies were seen in the acini (H&E, ×200). (B) Portal and periportal infiltration of lymphoid cells and a few plasma cells were seen. The bile ducts seemed to be intact (H&E, ×400). (C) Masson's trichrome staining revealed portal and periportal fibrosis with bridging (×100).
Reference
-
1. Czaja AJ, Souto EO, Bittencourt PL, et al. Clinical distinctions and pathogenic implications of type 1 autoimmune hepatitis in Brazil and the United States. J Hepatol. 2002. 37:302–308.2. Krawitt EL. Autoimmune hepatitis. N Engl J Med. 2006. 354:54–66.3. McFarlane IG. The relationship between autoimmune markers and different clinical syndromes in autoimmune hepatitis. Gut. 1998. 42:599–602.4. Homberg JC, Abuaf N, Bernard O, et al. Chronic active hepatitis associated with antiliver/kidney microsome antibody type 1: a second type of "autoimmune" hepatitis. Hepatology. 1987. 7:1333–1339.5. Gregorio GV, Portmann B, Reid F, et al. Autoimmune hepatitis in childhood: a 20-year experience. Hepatology. 1997. 25:541–547.6. West M, Jasin HE, Medhekar S. The development of connective tissue diseases in patients with autoimmune hepatitis: a case series. Semin Arthritis Rheum. 2006. 35:344–348.7. Youssef WI, Tavill AS. Connective tissue diseases and the liver. J Clin Gastroenterol. 2002. 35:345–349.8. Cohen S. The gastrointestinal manifestations of scleroderma: pathogenesis and management. Gastroenterology. 1980. 79:155–166.9. Bartholomew LG, Cain JC, Winkelmann RK, Baggenstoss AH. Chronic disease of the liver associated with systemic scleroderma. Am J Dig Dis. 1964. 9:43–55.10. Clarke AK, Galbraith RM, Hamilton EB, Williams R. Rheumatic disorders in primary biliary cirrhosis. Ann Rheum Dis. 1978. 37:42–47.11. Ishikawa M, Okada J, Shibuya A, Kondo H. CRST syndrome (calcinosis cutis, Raynaud's phenomenon, sclerodactyly, and telangiectasia) associated with autoimmune hepatitis. Intern Med. 1995. 34:6–9.12. Yabe H, Noma K, Tada N, Mochizuki S, Nagano M. A case of CREST syndrome with rapidly progressive liver damage. Intern Med. 1992. 31:69–73.13. Bernstein RM, Callender ME, Neuberger JM, Hughes GR, Williams R. Anticentromere antibody in primary biliary cirrhosis. Ann Rheum Dis. 1982. 41:612–614.14. Cassani F, Bianchi FB, Lenzi M, Volta U, Pisi E. Immunomorphological characterisation of antinuclear antibodies in chronic liver disease. J Clin Pathol. 1985. 38:801–805.15. Makinen D, Fritzler M, Davis P, Sherlock S. Anticentromere antibodies in primary biliary cirrhosis. Arthritis Rheum. 1983. 26:914–917.16. Johnson PJ, McFarlane IG. Meeting report: International Autoimmune Hepatitis Group. Hepatology. 1993. 18:998–1005.17. Steen VD, Medsger TA Jr. Case-control study of corticosteroids and other drugs that either precipitate or protect from the development of scleroderma renal crisis. Arthritis Rheum. 1998. 41:1613–1619.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Overlap Syndromebetween Autoimmune Hepatitis and Primary Biliary Cirrhosis
- A Case of Lupus-Related Hepatitis Mimicking Autoimmune Hepatitis
- Diffuse Systemic Sclerosis in a Patient with Primary Biliary Cirrhosis and Autoimmune Hepatitis Overlap Syndrome: A Case Report
- A Case of Autoimmune Hepatitis Associated with Systemic Lupus Erythematosus
- A Case of Autoimmune Hepatitis Combined with Ulcerative Colitis
