A Case of Primary Colon Amyloidosis Presenting as Hematochezia
- Affiliations
-
- 1Department of Internal Medicine, Kyungpook National University School of Medicine, Daegu, Korea. sw-jeon@hanmail.net
- KMID: 1775832
- DOI: http://doi.org/10.4166/kjg.2012.59.1.44
Abstract
- Amyloidosis is characterized by a deposition of insoluble fibrils in various organs and tissues. Amyloid deposition, in the gastrointestinal track, provokes a dysfunction of the organ, due to an accumulation of fibrils, and causes a variety of clinical symptoms and endoscopic findings. Primary amyloidosis in the gastrointestinal tract is rarely reported in Korea. We experienced a case of recurrent intestinal bleeding, in a 59-year-old female patient with primary amyloidosis. A colonoscopy revealed the presence of multiple large circular ulcers. In the entire colon, diffuse nodular lesions with edema and bleeding were found. A colonoscopic biopsy established the diagnosis of amyloidosis, to the exclusion of other disease components. We concluded that the patient had localized amyloidosis. Though a definitive therapeutic strategy has not been established for localized gastrointestinal amyloidosis, the patient has been successfully treated with a high-dose of steroids and azathioprine.
Keyword
MeSH Terms
Figure
-

Fig. 1 Abdominal CT findings. It demonstrated diffuse mural thickening in the ascending colon, transverse colon and descending colon.
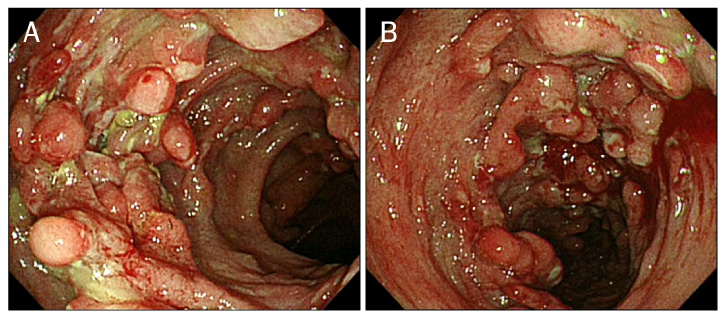
Fig. 2 Colonoscopic findings. (A) It demonstrated diffuse nodular lesions with bleeding and friability at the ascending colon. (B) It demonstrated multiple irregular large ulcers with nodular lesions at the descending colon.
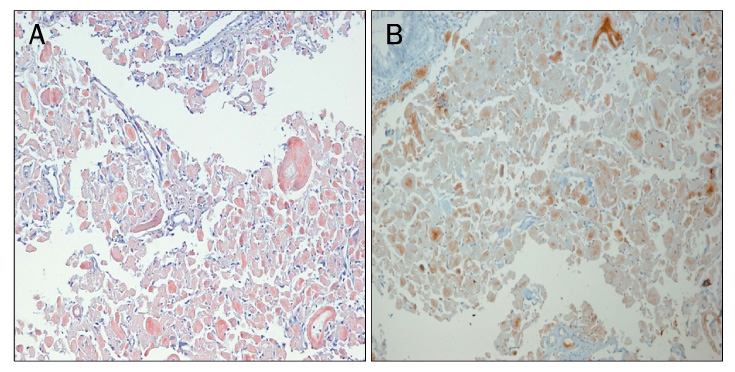
Fig. 3 Microscopic findings (Congo-red stain, ×100). (A) Congo-red stain revealed pink red deposits in the lamina propria of the colon. (B) The yellow-green birefringence of the deposits was observed by polarizing microscope.
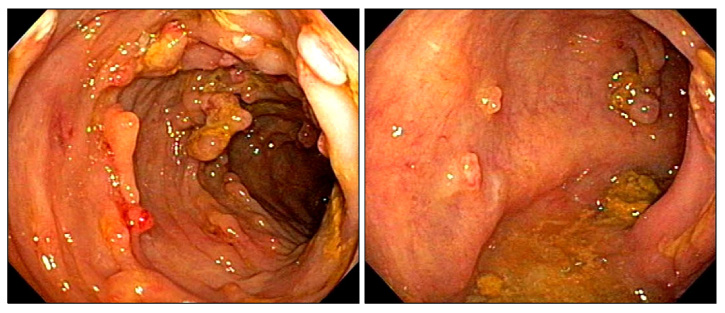
Fig. 4 Colonoscopic findings. Follow-up colonoscopy demonstrated improvement of diffuse nodular lesions and ulceration at the entire colon.
Cited by 1 articles
-
A Case of Primary Gastric Amyloidosis with Fulminant Heart Failure
Seonghun Hong, Young-Woon Chang, Jong Kyu Byun, Min Je Kim, Jung Min Chae, Sun Hee Park, Chi Hyuk Oh, Yong-Koo Park
Korean J Gastroenterol. 2015;66(4):227-230. doi: 10.4166/kjg.2015.66.4.227.
Reference
-
1. Scott PP, Scott WW Jr, Siegelman SS. Amyloidosis: an overview. Semin Roentgenol. 1986. 21:103–112.2. Kyle RA, Bayrd ED. Amyloidosis: review of 236 cases. Medicine (Baltimore). 1975. 54:271–299.3. Glenner GG, Ein D, Terry WD. The immunoglobulin origin of amyloid. Am J Med. 1972. 52:141–147.4. Gertz MA, Lacy MQ, Dispenzieri A, Hayman SR. Amyloidosis. Best Pract Res Clin Haematol. 2005. 18:709–727.5. Falk RH, Comenzo RL, Skinner M. The systemic amyloidoses. N Engl J Med. 1997. 337:898–909.6. Gertz MA, Comenzo R, Falk RH, et al. Definition of organ involvement and treatment response in immunoglobulin light chain amyloidosis (AL): a consensus opinion from the 10th International Symposium on Amyloid and Amyloidosis, Tours, France, 18-22 April 2004. Am J Hematol. 2005. 79:319–328.7. Moon W, Lee OY, Cho YJ, et al. The endoscopic findings and clinical characteristics of gastrointestinal amyloidosis. Korean J Gastrointest Endosc. 2005. 31:216–220.8. Leem JM, Choi JH, Park NG, et al. A case of gastrointestinal amyloidosis presenting with hematochezia. Korean J Gastrointest Endosc. 2002. 25:38–42.9. Levy DJ, Franklin GO, Rosenthal WS. Gastrointestinal bleeding and amyloidosis. Am J Gastroenterol. 1982. 77:422–426.10. Barth WF, Glenner GG, Waldmann TA, Zelis RF. Primary amyloidosis. Ann Intern Med. 1968. 69:787–805.11. Chitkara NL, Chugh TD, Chhuttani PN, Chugh KS. Secondary amyloidosis. Indian J Pathol Bacteriol. 1965. 8:285–293.12. Patel SA, al-Haddadin D, Schopp J, Cantave I, Duarte B, Watkins JL. Gastrointestinal manifestations of amyloidosis: a case of diverticular perforation. Am J Gastroenterol. 1993. 88:578–582.13. Puchtler H, Sweat F, Levine M. On the binding of congo red by amyloid. J Histochem Cytochem. 1962. 10:355–364.14. Usui M, Matsuda S, Suzuki H, Hirata K, Ogura Y, Shiraishi T. Gastric amyloidosis with massive bleeding requiring emergency surgery. J Gastroenterol. 2000. 35:924–928.15. Kyle RA, Gertz MA, Greipp PR, et al. A trial of three regimens for primary amyloidosis: colchicine alone, melphalan and prednisone, and melphalan, prednisone, and colchicine. N Engl J Med. 1997. 336:1202–1207.16. Takahashi A, Matsumoto J, Nishimura S, et al. Improvement of endoscopic and histologic findings of AA-type gastrointestinal amyloidosis by treatment with dimethyl sulfoxide and prednisolone. Gastroenterol Jpn. 1985. 20:143–147.17. Cohen HJ, Lessin LS, Hallal J, Burkholder P. Resolution of primary amyloidosis during chemotherapy. Studies in a patient with nephrotic syndrome. Ann Intern Med. 1975. 82:466–473.18. Redleaf PD, Davis RB, Kucinski C, Hoilund L, Gans H. Amyloidosis with and unusual bleeding diathesis; observations on the use of epsilon amino caproic acid. Ann Intern Med. 1963. 58:347–354.19. Nakamura T, Higashi S, Tomoda K, Tsukano M, Baba S. Efficacy of etanercept in patients with AA amyloidosis secondary to rheumatoid arthritis. Clin Exp Rheumatol. 2007. 25:518–522.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Intestinal Hemorrhage in Patient with Primary Amyloidosis
- A Case of Amyloidosis with Recurrent Intestinal Bleeding
- A Case of Secondary Amyloidosis Presenting as Massive Gastrointestinal Bleeding
- Primary Systemic Amyloidosis Presenting as Swollen Dense Breast: A Case Report
- Primary localized amyloidosis of the bladder: a case report
